Ovarian cysts are incredibly common, affecting a vast number of women throughout their reproductive years. Most are functional, harmless, and resolve on their own without medical intervention. However, when a cyst grows beyond a certain threshold, it shifts from a minor clinical observation to a potential health concern that requires diligent monitoring or surgical intervention. Understanding what constitutes a “large” ovarian cyst is essential for both patient awareness and effective clinical management.
Defining the Threshold for Size
In the medical community, the categorization of a cyst’s size is not entirely binary. There is no singular, universal number that instantly labels a cyst as “large,” as the clinical significance is often tied to the patient’s age, menopausal status, and the presence of symptoms. However, diagnostic imaging—specifically transvaginal ultrasound—provides clear parameters used by gynecologists to dictate the course of action.
The 5-Centimeter Benchmark
Generally, clinical guidelines often cite 5 centimeters (approximately 2 inches) as a common threshold for monitoring. Cysts smaller than 5 centimeters are frequently classified as small or incidental findings. They are often follicular or corpus luteum cysts that will likely disappear during a subsequent menstrual cycle. When a cyst reaches or exceeds the 5-centimeter mark, it is often considered large enough to warrant closer scrutiny or follow-up imaging in a few months to ensure it has not grown or persisted.
The 10-Centimeter “Giant” Classification
When a cyst reaches 10 centimeters (approximately 4 inches) in diameter, it enters the category of a “large” or, in clinical terminology, a “giant” ovarian cyst. At this size, the mass is significant enough to cause anatomical displacement of surrounding pelvic organs. It may become palpable during a routine physical examination and is much less likely to resolve spontaneously. These large masses are frequently associated with higher risks of complications, such as torsion or rupture, necessitating a more proactive surgical approach.
Clinical Implications of Large Ovarian Cysts
When a cyst moves from the “small” category into the “large” category, the physiological impact on the body changes. Size often correlates with a higher risk of physical symptoms and mechanical complications.
Mechanical Pressure and Symptoms
As a cyst expands, it occupies space within the pelvic cavity that is otherwise reserved for the bladder, bowel, and uterus. This encroachment often leads to distinct clinical symptoms:
- Abdominal Distension: Patients may notice a visible increase in abdominal girth or a feeling of fullness.
- Urinary Frequency: Compression of the bladder reduces its capacity, leading to frequent urges to urinate.
- Bowel Changes: Pressure on the rectum or colon can lead to constipation or a feeling of incomplete bowel evacuation.
- Pelvic Pain: Large cysts may cause a persistent, dull ache or sharp, episodic pain as they press against pelvic nerves or blood vessels.
Complications: Torsion and Rupture
Size is a significant risk factor for ovarian torsion—a medical emergency where the ovary twists around its ligamentous support, cutting off blood supply. A larger, heavier cyst increases the likelihood of the ovary becoming unstable and twisting. Furthermore, very large cysts have thinner walls relative to their volume, increasing the risk of spontaneous rupture. A rupture can cause internal bleeding and severe, acute pain, requiring immediate emergency care.
Diagnostic Evaluation and Differentiation

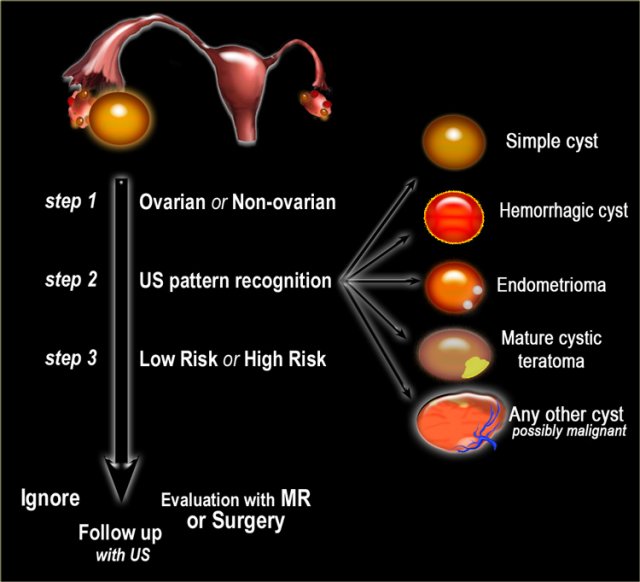
Identifying the size of a cyst is only the first step. For a clinician, the “largeness” of a cyst is secondary to the question of its nature. Is it a simple fluid-filled sac, or is it a complex mass with potential malignancy?
The Role of Ultrasound and MRI
Transvaginal ultrasound is the gold standard for initial assessment. It allows radiologists to measure the cyst in three dimensions and evaluate its internal structure. A “simple” cyst is anechoic (meaning sound waves pass through without echoing) and has thin, smooth walls. A “complex” cyst contains septations, solid components, or irregular borders. As a cyst increases in size, the importance of distinguishing between simple and complex morphology becomes paramount. If an ultrasound is inconclusive, a pelvic MRI is often ordered to provide a more detailed map of the tissues, which is particularly useful for very large cysts that may obscure surrounding anatomy on a standard ultrasound.
Serum Biomarkers
While size is the primary physical concern, blood tests—specifically CA-125—are often used in conjunction with imaging for large cysts. While CA-125 is not a perfect screening tool for ovarian cancer (as it can be elevated by benign conditions like endometriosis or fibroids), it acts as a secondary data point. In postmenopausal women, a large cyst coupled with an elevated CA-125 level significantly increases the clinical suspicion of malignancy, necessitating surgery by a gynecologic oncologist.
Treatment Pathways for Large Cysts
Once a cyst is confirmed to be large, the treatment strategy is determined by the patient’s age and the structural characteristics of the mass.
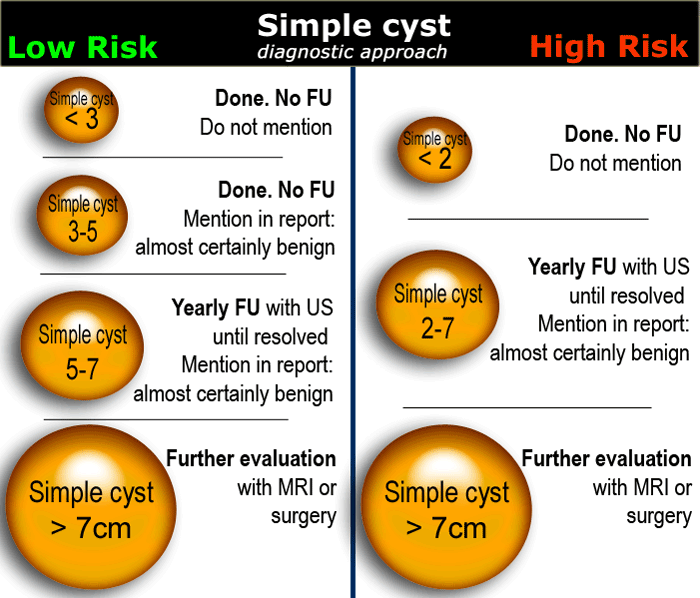
Observation and Serial Imaging
If a large cyst appears “simple” on an ultrasound and the patient is asymptomatic, some clinicians may opt for a period of “watchful waiting.” This involves serial ultrasounds every 3 to 6 months to check for stability. If the cyst remains static in size and the patient remains asymptomatic, some women may choose to avoid surgical intervention. However, this is usually only an option for premenopausal patients who show no signs of malignancy.
Surgical Intervention: Cystectomy vs. Oophorectomy
When a large cyst causes persistent pain, shows signs of growth, or displays complex features on imaging, surgery is generally indicated. There are two primary surgical approaches:
- Ovarian Cystectomy: This procedure involves removing the cyst while leaving the healthy ovarian tissue intact. This is the preferred method for women of reproductive age, as it preserves fertility and hormonal function.
- Oophorectomy: This involves the removal of the entire ovary. This is often necessary if the cyst is so large that it has replaced the entire ovary, or if the patient is postmenopausal and the risks of malignancy are higher.
Advancements in surgical technology have made these procedures increasingly common via minimally invasive techniques, such as laparoscopy or robotic-assisted surgery. These methods allow for smaller incisions, reduced recovery times, and less post-operative pain compared to traditional open laparotomy, even when dealing with surprisingly large masses.
The Importance of Professional Guidance
Determining whether an ovarian cyst is “large” is a nuanced process that requires professional medical evaluation. Because ovarian health is so closely tied to hormonal balance and fertility, self-diagnosis or dismissal of symptoms can be detrimental.
If you suspect you have an ovarian cyst—perhaps due to pelvic fullness, bloating, or irregular cycles—it is vital to schedule an examination with a gynecologist. Imaging is the only way to accurately measure a cyst and assess its risks. While the term “large ovarian cyst” sounds intimidating, modern medicine offers sophisticated tools to monitor these growths and effective surgical options to remove them when necessary. With proper care and timely intervention, most women successfully navigate these findings and maintain their long-term gynecological health. Never ignore persistent pelvic symptoms; early detection of a large cyst allows for more conservative treatment options and better clinical outcomes.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.