The seemingly simple act of drawing blood for a Complete Blood Count (CBC) is underpinned by a sophisticated interplay of chemical engineering, precision instrumentation, and advanced digital systems. The choice of collection tube, particularly its cap color, signifies a critical technical specification that directly impacts the integrity of the sample and the accuracy of diagnostic results. For a CBC, the purple-topped tube is the industry standard, a choice dictated by the precise scientific requirements of hematology analysis and integrated into the complex technological ecosystem of modern clinical laboratories.
The Core Technology: Anticoagulants and Blood Sample Integrity
At the heart of the “purple tube” selection lies the advanced chemical technology of its anticoagulant. Understanding this technology is paramount for grasping why this specific tube is indispensable for CBC analysis.
Understanding EDTA: The Purple Powerhouse
The purple-capped tube contains ethylenediaminetetraacetic acid (EDTA), a chelating agent that plays a crucial technical role in preserving blood samples for hematological studies. EDTA works by irreversibly binding to calcium ions, which are essential cofactors in the coagulation cascade. By effectively sequestering calcium, EDTA prevents blood from clotting. This anti-coagulation mechanism is vital for CBCs because the test requires the blood cells—red blood cells, white blood cells, and platelets—to remain in their natural, unbound state, allowing automated analyzers to count, size, and differentiate them accurately.
The technical brilliance of EDTA lies in its ability to prevent clotting without significantly altering cellular morphology or interfering with the various cell components for a critical period. Other anticoagulants, while effective for different tests, might cause cellular shrinkage (e.g., heparin can interfere with some staining), induce platelet clumping, or alter cell indices, thus compromising the accuracy of the CBC. The specific concentration of EDTA in these tubes is also meticulously calibrated to ensure optimal anticoagulation without causing adverse effects like cell crenation or dilution artifacts, which would technically invalidate the results.
Beyond the Purple: The Spectrum of Tube Technologies
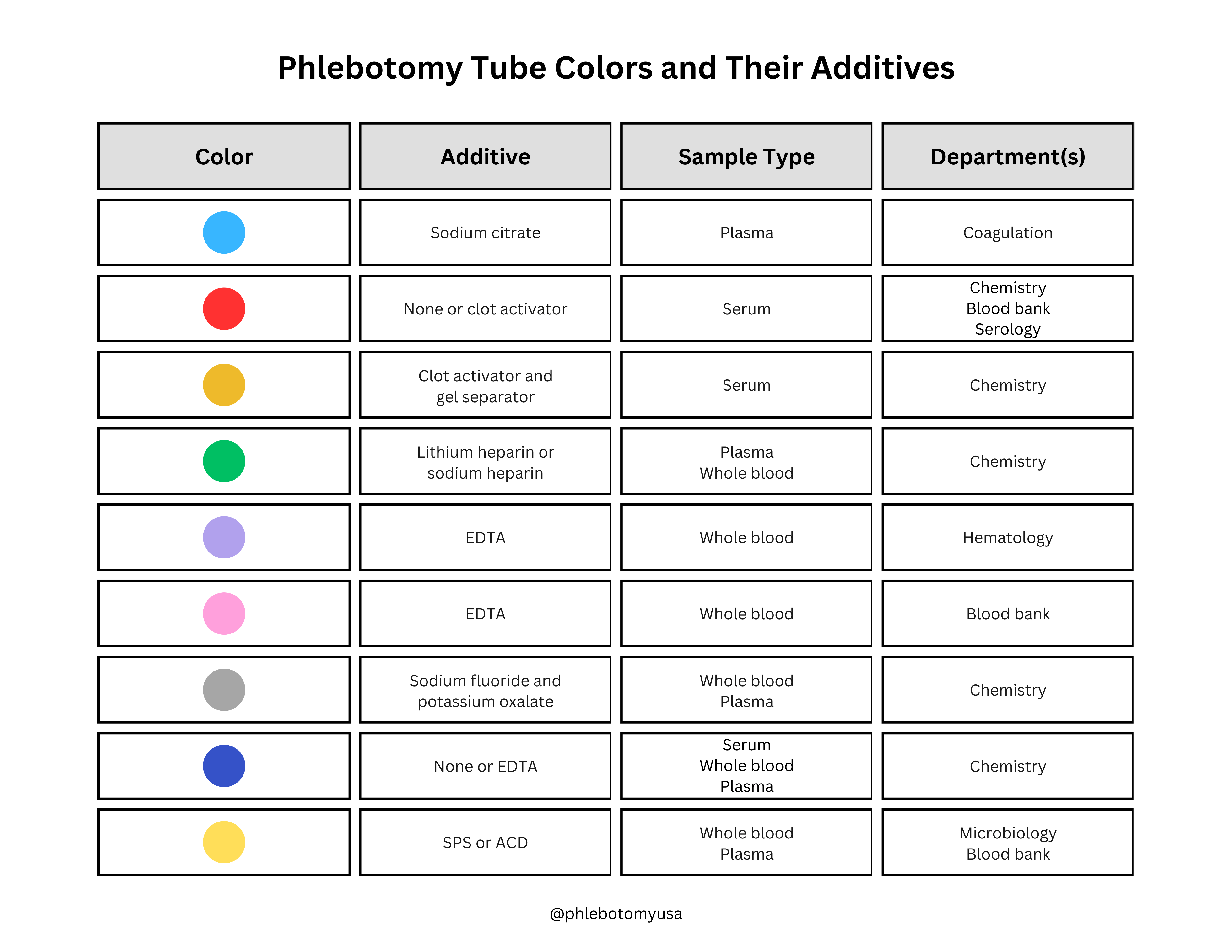
While purple is the color for CBC, it’s crucial to acknowledge the broader spectrum of tube technologies, each designed with specific technical requirements in mind. For instance, light blue-capped tubes contain sodium citrate, a weaker calcium chelator, specifically formulated for coagulation studies where the ratio of anticoagulant to blood is critically important for accurate assessment of clotting factors. Green-capped tubes contain heparin (lithium, sodium, or ammonium heparin), which inhibits thrombin, suitable for plasma chemistry tests but generally not ideal for hematology due to potential cellular clumping and interference with Wright’s stain. Red-topped or gold-topped tubes typically contain clot activators or gel separators for serum chemistry, where the absence of anticoagulant allows the blood to clot, yielding serum.
The diversity of tube technologies underscores the principle that each diagnostic test has unique technical prerequisites. The wrong tube, even with blood, is a technically unsuitable sample for a given test, leading to potential re-draws and diagnostic delays. The choice of the purple tube for CBC, therefore, is not arbitrary but a scientifically and technically informed decision based on EDTA’s superior capability to preserve cellular components for accurate hematological analysis.
The Critical Role of Proper Filling and Mixing Technologies
Even with the correct EDTA tube, the technical integrity of the sample can be compromised by improper collection techniques. Most EDTA tubes are designed for a specific volume of blood, ensuring an optimal blood-to-anticoagulant ratio. Underfilling can lead to an excess of EDTA relative to blood, causing cell shrinkage, false decreases in hematocrit, and morphological changes. Overfilling, conversely, can dilute the EDTA concentration, leading to microclots that can jam automated analyzers and produce erroneous cell counts.
Modern phlebotomy practices emphasize precise filling, often guided by line indicators on the tube. Following collection, immediate and gentle inversion (typically 8-10 times) is critical. This manual mixing, sometimes augmented by automated tube rockers in high-volume settings, ensures the EDTA is thoroughly dispersed throughout the blood sample, preventing localized clotting without causing hemolysis or cell damage. This meticulous attention to detail in the pre-analytical phase is a technical safeguard against analytical errors, ensuring the sample presented to the automated analyzer is as close to its in-vivo state as possible.
Automation and Digital Integration: Ensuring Accuracy in CBC Analysis
The correct tube color and proper collection techniques lay the groundwork for accurate CBC analysis, but the real power of modern diagnostics comes from sophisticated automation and seamless digital integration within the laboratory.
Automated Hematology Analyzers: The Brains Behind the Count
Automated hematology analyzers are marvels of biomedical engineering, representing the pinnacle of laboratory technology for CBC analysis. These instruments precisely aspirate a small volume of blood from the EDTA tube and employ a combination of impedance, optical light scatter, and cytochemical staining technologies to enumerate and differentiate blood cells.
When an EDTA tube arrives at the analyzer, its barcode is scanned, digitally linking the sample to the patient’s record in the Laboratory Information System (LIS). This automated identification eliminates manual transcription errors. The analyzer then uses sophisticated fluidics to dilute and mix the sample accurately. For cell counting, the impedance method measures changes in electrical resistance as cells pass through an aperture, while optical light scatter (flow cytometry) uses laser technology to measure cell size, internal complexity, and granularity. These advanced sensors and algorithms can count thousands of cells per second, providing highly precise data on red blood cell count (RBC), white blood cell count (WBC), platelet count (PLT), hemoglobin (Hgb), hematocrit (Hct), and various cellular indices (MCV, MCH, MCHC, RDW). Furthermore, advanced analyzers can perform a WBC differential, classifying neutrophils, lymphocytes, monocytes, eosinophils, and basophils based on their unique light scatter patterns and staining properties, significantly enhancing diagnostic utility.
Laboratory Information Systems (LIS): The Digital Backbone
The Laboratory Information System (LIS) is the digital nexus that orchestrates the entire workflow from test ordering to result reporting. For CBC analysis, the LIS plays a critical role in data integrity, workflow automation, and quality control. When a physician orders a CBC, the LIS generates a unique accession number and a corresponding barcode, often specifying the “purple tube” requirement.

Upon sample collection, the LIS tracks the tube’s journey from phlebotomy to analysis. It receives real-time data from automated hematology analyzers, integrating raw counts and differentials into the patient’s electronic health record. The LIS employs sophisticated algorithms to flag abnormal results, trigger reflex testing protocols, or indicate potential instrument errors, prompting technical review by laboratory professionals. This digital integration ensures that critical data points are never manually transcribed, minimizing human error and accelerating the availability of results. Beyond individual patient samples, the LIS also aggregates data for quality control, instrument performance monitoring, and epidemiological tracking, offering a comprehensive digital platform for laboratory management and oversight.
Minimizing Pre-Analytical Errors Through Tech Protocols
Pre-analytical errors—those occurring before the sample reaches the analyzer—are the most common source of diagnostic inaccuracy. Technology plays a pivotal role in minimizing these errors. Digital checklists and standard operating procedures (SOPs) accessible via tablets or computers guide phlebotomists through the correct tube selection and collection sequence. Barcode scanning at the point of collection ensures that the correct patient is being drawn and that the sample is matched to the correct order.
Advanced LIS systems can track phlebotomy performance, identifying trends in rejected samples due to incorrect tubes or inadequate filling. Training modules, often interactive and multimedia-rich, utilize technology to educate staff on the technical nuances of blood collection. Moreover, instrument error flags, automatically generated by analyzers and integrated into the LIS, alert technicians to potential sample quality issues (e.g., clots, hemolysis) that might stem from pre-analytical missteps, enabling timely intervention and preventing the release of erroneous results.
The Impact of Technical Deviations: Data Integrity and Patient Outcomes
While technology provides robust systems for CBC analysis, any deviation from established technical protocols, particularly regarding tube selection, can have significant repercussions on data integrity and, by extension, patient outcomes.
Consequences of Incorrect Tube Selection
Using the wrong tube color for a CBC leads to a cascade of technical issues. If, for example, a heparinized (green top) tube is used instead of an EDTA (purple top) tube, the heparin might cause platelets to clump, leading to spuriously low platelet counts and potentially triggering unnecessary investigations for thrombocytopenia. Heparin can also interfere with cellular staining, making microscopic review challenging. Using a serum separator tube (gold top) would result in a clotted sample, rendering it completely unsuitable for CBC analysis as cells would be trapped within the fibrin matrix, making accurate counting impossible.
These technical interferences result in “flags” from automated analyzers, requiring manual intervention, sample rejection, and ultimately, a redraw. This not only delays diagnosis but also imposes additional stress on the patient and consumes valuable laboratory resources. The entire analytical process, designed for the specific technical properties of an EDTA sample, fails when the foundational technical requirement—the correct tube and anticoagulant—is not met.
The Cost of Technical Errors: Time, Resources, and Redraws
The operational and financial implications of technical errors in sample collection are substantial. Each redraw represents a significant waste of time for both patients and healthcare staff. A phlebotomist must spend additional time recollecting the sample, potentially disrupting their schedule. The laboratory incurs the cost of another tube, additional reagents, and repeated analysis time on expensive instrumentation. More critically, delayed results can impact patient care, postponing critical treatment decisions or prolonging hospital stays. For high-volume laboratories, even a small percentage of redraws due to incorrect tube usage can accumulate into substantial financial losses and operational bottlenecks. The technical precision required at the collection stage directly translates into efficiency and cost-effectiveness downstream in the diagnostic process.
Quality Assurance Technologies in Hematology
To mitigate these risks, modern laboratories heavily rely on comprehensive quality assurance (QA) technologies. Internal Quality Control (IQC) involves running known control samples with established ranges through analyzers multiple times a day. The data generated from these runs is analyzed by sophisticated software that employs statistical algorithms (e.g., Levey-Jennings charts) to monitor instrument performance and detect subtle technical shifts or trends. External Quality Assessment (EQA) or proficiency testing programs involve laboratories analyzing unknown samples provided by external agencies. The results are compared against peer groups, providing an independent verification of the laboratory’s technical accuracy and compliance with global standards. These robust QA systems, powered by advanced software and statistical analysis, ensure that the entire CBC testing process, from sample reception to result reporting, consistently meets the highest technical standards.
Future Tech: Advancements in Blood Collection and Analysis
The field of clinical diagnostics is continuously evolving, driven by technological innovation. The future promises even more advanced solutions for blood collection and analysis, further enhancing accuracy and efficiency.
Smart Tubes and Digital Tracking
Imagine “smart” collection tubes embedded with micro-RFID chips or advanced QR codes that contain not just patient data but also real-time information about the sample’s journey, temperature fluctuations, and even agitation levels. These tubes could communicate directly with the LIS and automated analyzers, providing an unparalleled level of digital tracking and quality assurance from the point of collection. This technology could automatically flag samples that have been improperly handled or experienced conditions that might compromise their integrity, leading to proactive intervention rather than retrospective error detection.
Point-of-Care Testing (POCT) Innovations
Point-of-Care Testing (POCT) devices for CBCs are also becoming more sophisticated. While current POCT devices may not offer the full differential capabilities of central lab analyzers, advancements in microfluidics, lab-on-a-chip technology, and miniaturized sensor arrays are making highly accurate, comprehensive CBCs possible closer to the patient. These devices will still rely on the fundamental chemical engineering principles of anticoagulation but will integrate advanced data processing and connectivity to relay results securely and quickly to the patient’s electronic health record, offering rapid diagnostic insights in emergency settings or remote locations.

The Role of AI and Machine Learning in Hematology Diagnostics
Artificial intelligence (AI) and machine learning (ML) are poised to revolutionize hematology diagnostics. AI algorithms can be trained on vast datasets of blood smear images to autonomously identify and classify abnormal cells with unprecedented speed and accuracy, augmenting the expertise of human morphologists. Predictive analytics can analyze LIS data to forecast instrument maintenance needs, optimize workflow, and even identify subtle patterns in patient results that might indicate emerging health concerns. AI could also play a role in optimizing phlebotomy training through virtual reality simulations, providing instant feedback on technique, thereby reducing pre-analytical errors at the source. These AI-driven tools promise to enhance diagnostic efficiency, improve turnaround times, and ultimately lead to more personalized and precise patient care within the complex technological landscape of the modern laboratory.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.