The human brain is an architectural marvel of biological engineering, containing structures that often go unnoticed until clinical imaging brings them to the forefront of medical curiosity. Among these, the cavum septum pellucidum (CSP) stands out as a fascinating anatomical feature that bridges the gap between developmental biology and neuro-radiology. While it is often discussed in the context of fetal development and psychiatric research, it remains a topic shrouded in common misconceptions for the layperson. Understanding the CSP requires a deep dive into the midline structures of the brain and the developmental timeline that defines human neuroanatomy.

The Anatomical Foundation of the Septum Pellucidum
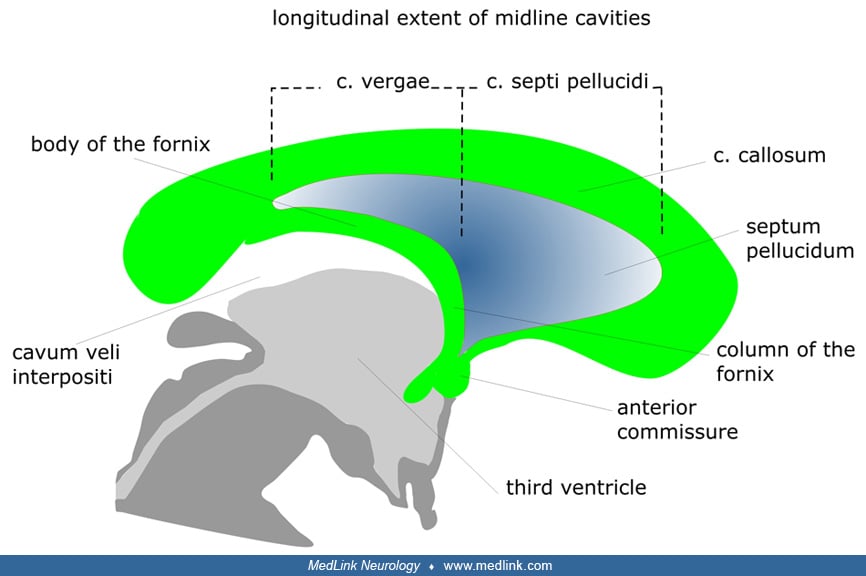
To understand what the cavum septum pellucidum is, one must first identify the septum pellucidum itself. The septum pellucidum is a thin, triangular, double-layered membrane that runs vertically down the middle of the brain. It acts as a structural partition, separating the lateral ventricles—the fluid-filled cavities responsible for the circulation of cerebrospinal fluid—from one another.
Defining the Cavum
The “cavum” refers to the space that exists between these two layers. In the early stages of fetal development, this space is a normal, fluid-filled gap. As the brain matures and the corpus callosum—the thick bundle of nerve fibers connecting the two hemispheres—develops, this gap typically closes. When the space persists beyond infancy, it is referred to as a cavum septum pellucidum.
Developmental Variations
It is important to distinguish between a “pathological” finding and a normal anatomical variant. In the vast majority of cases, the presence of a CSP in an adult is considered a benign neuro-anatomical variant. It is not necessarily a sign of brain damage or developmental delay, but rather a reflection of the unique, individual way in which a specific brain completed its prenatal maturation.
Clinical Significance and Neuroimaging Findings
In the modern era of medicine, the identification of a CSP is almost exclusively a byproduct of advanced neuroimaging. With the widespread use of magnetic resonance imaging (MRI) and computed tomography (CT) scans for investigating headaches, trauma, or neurological symptoms, radiologists frequently encounter the CSP as an incidental finding.
Why Imaging Matters
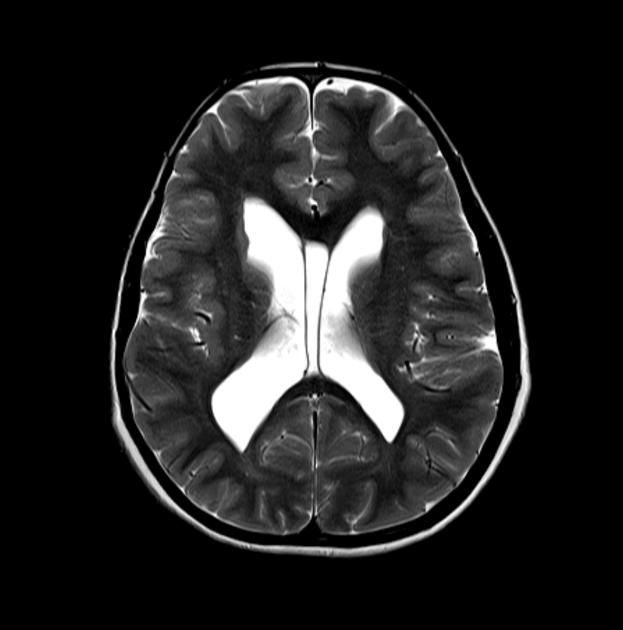
When a patient undergoes an MRI, the radiologist looks for symmetry and the absence of mass effect. A cavum septum pellucidum appears as a clear, fluid-filled space between the lateral ventricles. Because it follows the signal intensity of cerebrospinal fluid on an MRI, it is easily distinguished from tumors, cysts, or other space-occupying lesions. Recognizing this structure prevents unnecessary alarm or medical intervention, as a simple CSP is, in isolation, clinically silent.
Distinguishing from the Cavum Vergae
Clinicians often look for the presence of the cavum vergae in conjunction with the CSP. While the CSP is located anteriorly, the cavum vergae is a posterior extension of that same space. The two are often continuous, and their clinical implications—or lack thereof—are functionally identical. Both are categorized as developmental remnants that carry no intrinsic morbidity for the vast majority of the population.
The Intersection of Neuroscience and Neuropsychiatry
For decades, the neuroscientific community has explored the relationship between midline brain structures and various neuropsychiatric conditions. This has led to intense academic debate regarding the “marker” status of the CSP.
Historical Context and Research
In the mid-20th century, researchers began measuring the size and presence of the CSP in patients with schizophrenia and other neurodevelopmental disorders. Some early studies hypothesized that a larger-than-average CSP might serve as a soft neurological marker for impaired fetal development. Because the septum pellucidum develops in tandem with the limbic system—a key area for emotional regulation and memory—scientists sought to determine if its persistence was linked to cognitive or emotional dysfunction.
Modern Scientific Consensus
Contemporary consensus has largely tempered these early associations. While statistical correlations have been observed in certain populations, they are frequently weak and inconsistent across larger, diverse cohorts. It is now widely accepted that a cavum septum pellucidum, regardless of its size, is not a diagnostic tool for psychiatric illness. Current neurology emphasizes that the structural morphology of the brain is incredibly diverse; what works for one healthy brain may look structurally different in another. Therefore, the presence of a CSP is not a predictor of functional impairment, intelligence, or mental health outcomes.
Life with a Cavum Septum Pellucidum: Common Questions
For individuals who receive a radiology report mentioning a cavum septum pellucidum, the experience can be disconcerting. Medical jargon often carries an inherent weight, and patients frequently worry that an “anatomical variant” implies a health risk.
Addressing Patient Anxiety
The most important takeaway for those discovering they have a CSP is that it is a common finding. Autopsy studies and large-scale imaging databases suggest that a significant percentage of the population—estimates range from 10% to 20% or even higher depending on the criteria used—possess some form of a persistent cavum septum pellucidum. It is a “normal” part of their brain’s unique blueprint.
When to Seek Consultation
Generally, a physician will not suggest further testing based on the discovery of a CSP alone. The structure does not grow, it does not exert pressure on surrounding tissue, and it does not impede the flow of cerebrospinal fluid unless it becomes exceptionally large or inflamed—a condition so rare that it is virtually unheard of in clinical practice. If a patient is undergoing imaging for a specific issue, such as migraine or post-concussion syndrome, the CSP is simply noted in the report as an incidental, benign finding. The focus of the clinician will remain on the underlying reason for the scan, rather than the stable, historical footprint of the CSP.
Conclusion: The Perspective of Biological Variation
The human brain is not manufactured according to a rigid, uniform template. From the gyral patterns of the cortex to the specific pathways of the white matter tracts, biological variation is the rule, not the exception. The cavum septum pellucidum is a quintessential example of this architectural diversity. It serves as a vestige of our early developmental history—a reminder of the intricate processes that occur in the womb to shape the organ of the mind.
By viewing the CSP through the lens of modern neuroscience, we move away from outdated notions of “pathology” and toward a more sophisticated appreciation for human anatomical variety. It is a structural signature, a testament to the fact that while our brains share a common functional design, they are uniquely individual in their physical manifestation. For the overwhelming majority of people, the cavum septum pellucidum is simply there, occupying a quiet space in the midline, exerting no influence on the complex thoughts, emotions, and experiences that define a person’s life. As medical imaging continues to improve, our understanding of these minor variants will continue to deepen, reinforcing the importance of context in interpreting the complex maps of the human brain.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.