In the modern clinical landscape, the detection of chemical compounds within the human body is no longer a simple “litmus test” procedure. It has evolved into a sophisticated branch of biotechnology, relying on complex sensors, automated algorithms, and high-resolution analytical hardware. Buprenorphine, a semi-synthetic opioid used extensively in medication-assisted treatment (MAT), represents one of the most technically challenging molecules to track accurately. While the technology governing urine drug screening (UDS) is remarkably advanced, it is not infallible. When we speak of a “false positive” for buprenorphine, we are essentially discussing a failure in the technological stack—a mismatch between the chemical input and the digital or enzymatic sensor’s interpretation.
To understand what causes these inaccuracies, we must look beyond the biology and examine the engineering, the software thresholds, and the signal-to-noise ratios that define modern laboratory diagnostics.
The Hardware of Detection: Immunoassay vs. Mass Spectrometry
The primary reason false positives occur in buprenorphine testing lies in the tiered technological approach used by most laboratories. Not all testing hardware is created equal; the industry generally relies on two distinct levels of technological sophistication: the initial screening (immunoassay) and the confirmatory analysis (Chromatography-Mass Spectrometry).
The Limitations of Initial Screen Technology
The initial screen is typically an Enzyme-Linked Immunosorbent Assay (ELISA) or a Kinetic Interaction of Microparticles in Solution (KIMS). This hardware functions as a high-speed, automated sensor designed for volume rather than absolute precision. In these systems, synthetic antibodies are programmed to “bind” to the buprenorphine molecule. If a binding event occurs, a signal is generated—much like a digital sensor detecting a specific frequency.
The technical flaw here is “cross-reactivity.” The antibody is essentially a biological sensor with a specific geometric requirement. If another molecule with a similar structural “shape” enters the sensor’s field, it can trigger a binding event, leading the software to report a positive result. This is a hardware limitation where the sensor cannot distinguish between the target analyte and a structurally similar “imposter” molecule.
Enzyme-Linked Immunosorbent Assay (ELISA) Interference
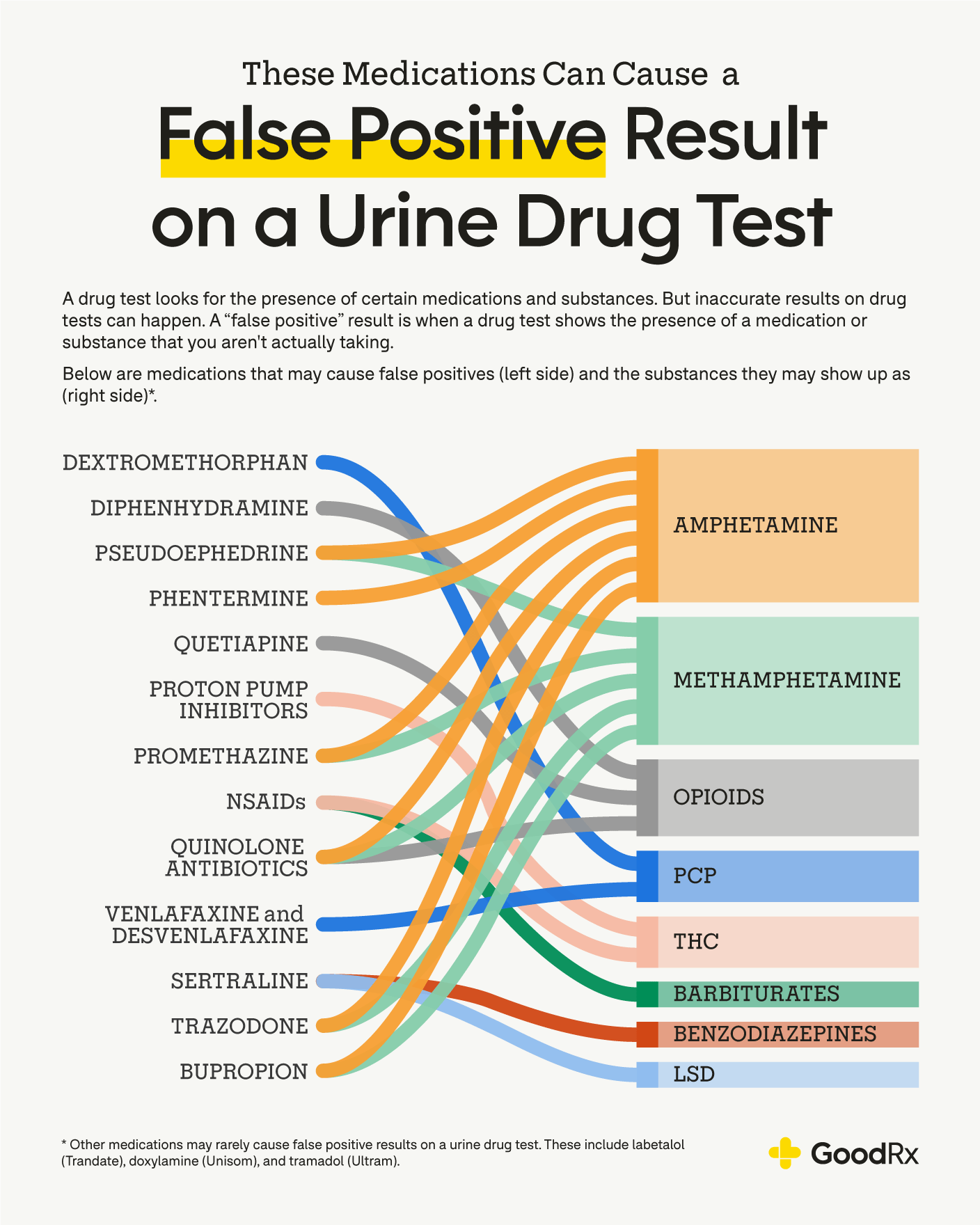
ELISA platforms are integrated into large-scale Laboratory Information Systems (LIS) that process thousands of samples daily. Because these systems are optimized for speed, they often operate with a lower “signal-to-noise” resolution. Certain medications—such as the antipsychotic Quetiapine (Seroquel) or the antihistamine Diphenhydramine (Benadryl)—can act as biological “noise.” When present in high concentrations, these substances can interfere with the enzymatic reaction on the ELISA plate, causing the hardware to output a digital signal that the LIS interprets as buprenorphine.
Signal Noise and Cross-Reactivity in the Digital Signature
In the world of signal processing, a false positive is often the result of “noise” being misinterpreted as a meaningful signal. In buprenorphine testing, this noise stems from chemical analogues and the sensitivity settings of the analytical software.
Chemical Analogues and Structural Overlap
The technical challenge of identifying buprenorphine is that it shares structural characteristics with other opioids and non-opioid medications. When a laboratory sets up its testing parameters, it must define the “molecular signature” it is looking for. However, certain drugs have a high degree of structural overlap.
For example, Tramadol or even certain cough suppressants can sometimes trigger a low-level response on older immunoassay hardware. From a tech perspective, this is a “false-trigger” error. The sensor’s “mask” for buprenorphine is too broad, allowing other molecules to fit into the detection window. This is particularly common in older, “point-of-care” (POC) testing kits, which lack the advanced filtration and data processing capabilities of centralized laboratory mainframes.
The Impact of High-Sensitivity Thresholds in Automated Systems
Software calibration plays a massive role in the accuracy of drug tests. Every automated testing system has a “cutoff” level—a digital threshold expressed in nanograms per milliliter (ng/mL). If the detected concentration is 10.1 ng/mL and the cutoff is 10.0 ng/mL, the software registers a “positive.”

The “false positive” often occurs when the threshold is set too low. High-sensitivity settings increase the “Recall” (finding all possible positives) but decrease “Precision” (the accuracy of those positives). If a patient is taking a legal medication that cross-reacts at a rate of 1%, and the software threshold is set to an ultra-sensitive level, that 1% noise is amplified into a positive result. This is a classic optimization problem in data science: balancing the risk of a false negative against the disruption caused by a false positive.
Software and Data Integration in Laboratory Information Systems (LIS)
Beyond the physical chemistry, the digital infrastructure of the laboratory itself can be a source of error. Modern toxicology relies on a complex “Chain of Custody” (CoC) that is managed entirely by software.
Algorithmic Calibration Errors
Mass spectrometry (the “gold standard” for confirmation) uses software to compare the mass-to-charge ratio of a sample against a known library of chemical signatures. If the library is not updated or if the calibration curve of the software has drifted, the system may misidentify a metabolite.
For instance, buprenorphine breaks down into norbuprenorphine. A sophisticated LIS must track both. If the software algorithm is programmed to flag any “unidentified peak” in the chromatography graph that falls within a certain retention time window, it might mislabel a completely unrelated compound as a buprenorphine metabolite. This is essentially a “bug” in the identification logic of the software.
Data Integrity and Chain-of-Custody Tracking
In any large-scale data processing environment, “garbage in, garbage out” remains a fundamental rule. False positives can occur through “data collision”—where a barcode error or a software glitch in the LIS assigns the results of one sample to the wrong patient ID. While this is not a “false positive” in the chemical sense, it is a technical failure of the data management system. Digital security protocols and robust hashing of patient data are the only ways to mitigate these administrative tech errors. Ensuring that the hardware (the analyzer) and the software (the LIS) are communicating via secure, error-correcting protocols is vital for result integrity.
The Future of Diagnostic Tech: AI and High-Resolution Mass Spectrometry
As we look toward the future of clinical technology, the industry is moving away from the error-prone “analog” sensors of the past and toward high-definition, AI-driven analysis.
Reducing False Positives through Machine Learning
The next generation of laboratory hardware will likely incorporate Machine Learning (ML) to analyze chromatography patterns. Instead of relying on a simple “binary” cutoff (positive/negative), ML algorithms can analyze the entire “landscape” of the urine sample. By training on millions of data points, these AI models can recognize the subtle difference between the “signal” of buprenorphine and the “noise” of a cross-reacting antidepressant. This represents a shift from “rule-based” software to “pattern-recognition” software, which significantly reduces the incidence of false positives.
Real-time Bio-monitoring and Wearable Tech
We are also seeing a shift toward “Point-of-Need” technology. Research into biosensors—small, wearable devices that can detect metabolites in sweat or interstitial fluid—is accelerating. These devices use microfluidics and nanotechnology to provide real-time data. Unlike a one-time urine test, which provides a “snapshot” prone to sensor noise, wearable tech provides a “stream” of data. This allows for “temporal verification”—if a sensor detects a sudden, unexplained spike that doesn’t fit the pharmacokinetic profile of buprenorphine, the software can automatically flag it as a technical anomaly or an external interference, rather than a positive result.
Conclusion: The Technical Imperative
A false positive for buprenorphine is rarely a mystery of biology; it is almost always a measurable failure of technology. Whether it is a low-resolution immunoassay sensor being fooled by a structural analogue, a software algorithm with a poorly calibrated threshold, or a data integrity error within a Laboratory Information System, the root causes are technical.
As we continue to integrate AI, higher-resolution mass spectrometry, and more robust LIS protocols into the clinical workflow, the “false positive” will eventually become a legacy issue of an earlier technological era. For now, understanding the hardware and software limitations of the testing stack is the first step in ensuring that data—not noise—drives clinical decision-making. In the high-stakes world of medical diagnostics, precision isn’t just a goal; it’s a technical requirement.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.