The question “how much is the ACA?” is far more complex than a simple dollar figure. It doesn’t just refer to the premium an individual might pay for a health insurance plan. Instead, it encompasses a vast web of financial considerations: the cost to taxpayers, the burden on businesses, the savings to individuals, and the broader economic impact on the healthcare system and national debt. The Affordable Care Act (ACA), signed into law in 2010, fundamentally reshaped the American healthcare landscape, and understanding its financial implications requires a multifaceted approach that accounts for individual outlays, government subsidies, and systemic expenditures.
At its core, the ACA aimed to expand health insurance coverage, control healthcare costs, and improve consumer protections. While these goals have brought tangible benefits to millions, they come with a significant price tag, distributed across various stakeholders. This article delves into the financial intricacies of the ACA, examining its direct costs to individuals and the government, its economic impact, and how to assess its value against its monetary price.
Understanding the ACA’s Financial Structure
The ACA introduced a new framework for health insurance markets, blending individual responsibility with government support. The financial architecture is designed to make coverage accessible, particularly for those who historically struggled to afford it.
Individual Premiums and Deductibles
For individuals, the most tangible “cost” of the ACA is the monthly premium paid for a health insurance plan obtained through the state or federal marketplaces (exchanges). These premiums vary widely based on several factors:
- Age: Older individuals generally pay higher premiums.
- Geographic Location: Healthcare costs differ significantly by state and even within a state, influencing premiums.
- Tobacco Use: Smokers can face higher surcharges.
- Plan Type (Metal Tiers): Plans are categorized into Bronze, Silver, Gold, and Platinum tiers, reflecting the actuarial value (the average percentage of healthcare costs the plan is expected to cover). Bronze plans have lower premiums but higher deductibles and out-of-pocket maximums, while Platinum plans have higher premiums but lower out-of-pocket costs.
- Family Size: Premiums increase with the number of people covered under a single plan.
Beyond premiums, individuals also face deductibles, copayments, and coinsurance, which are their out-of-pocket responsibilities before insurance coverage fully kicks in. The ACA caps annual out-of-pocket maximums to protect consumers from catastrophic medical bills, but these can still be substantial, often running into several thousands of dollars, particularly for Bronze and Silver plans.
Government Subsidies: Tax Credits and Cost-Sharing Reductions
A significant component of the ACA’s financial design is the provision of government subsidies to make coverage more affordable for low- and middle-income individuals and families. These come in two primary forms:
- Premium Tax Credits (PTCs): These are refundable tax credits that can be used immediately to lower monthly insurance premiums. Eligibility for PTCs is based on household income relative to the federal poverty level (FPL), ranging from 100% to 400% FPL (with temporary expansions increasing this threshold for many, as seen with the American Rescue Plan Act and Inflation Reduction Act). The amount of the credit is calculated on a sliding scale, ensuring that individuals and families pay no more than a certain percentage of their income for a benchmark Silver plan. This mechanism is crucial for reducing the upfront cost of insurance.
- Cost-Sharing Reductions (CSRs): Available only with Silver plans, CSRs help eligible individuals (typically those with incomes between 100% and 250% FPL) reduce their out-of-pocket costs, such as deductibles, copayments, and coinsurance. While the government stopped directly funding CSRs to insurers in 2017, many states and insurers implemented “silver loading,” where the cost of CSRs is loaded onto Silver plan premiums, indirectly continuing the benefit for eligible enrollees through higher PTCs.
These subsidies dramatically alter the effective cost of insurance for millions, making coverage attainable for populations who might otherwise be uninsured.
Medicaid Expansion
Another cornerstone of the ACA’s cost structure is the expansion of Medicaid eligibility. The ACA allowed states to expand Medicaid coverage to nearly all non-elderly adults with incomes up to 138% of the FPL. The federal government initially covered 100% of the cost for newly eligible individuals, gradually decreasing to 90% in subsequent years, with states picking up the remaining 10%. This expansion represents a substantial federal investment in healthcare for the nation’s lowest-income population. For states that have expanded Medicaid, it has significantly reduced rates of uninsurance and uncompensated care costs for hospitals, shifting a large portion of the financial burden from state and local governments (and uninsured individuals) to the federal budget.
The Broader Economic Impact: Who Pays and How?
The ACA’s costs extend beyond individual premiums and government subsidies to include various taxes, fees, and regulatory requirements that impact businesses, industries, and the national economy.
Funding Mechanisms: Taxes and Fees
To fund the expansion of coverage and other provisions, the ACA included several revenue-generating measures:
- Net Investment Income Tax (NIIT): A 3.8% tax on investment income for high-income earners.
- Additional Medicare Tax: A 0.9% increase in Medicare payroll taxes for high-income earners.
- Cadillac Tax (Repealed): A 40% excise tax on high-cost employer-sponsored health coverage, intended to curb excessive healthcare spending, but ultimately repealed before it took effect due to widespread opposition.
- Medical Device Excise Tax (Repealed): A 2.3% tax on the sale of certain medical devices, also later repealed.
- Annual Fee on Health Insurance Providers: An annual fee levied on health insurers based on their market share, designed to help fund the ACA’s coverage provisions. This fee was suspended and later repealed, though its impact was felt during its operational years.
- Employer Mandate Penalties: Large employers (50 or more full-time equivalent employees) are required to offer affordable health coverage to their full-time employees or face penalties. While not a tax, these penalties represent a revenue source for the government and a cost consideration for businesses.
These funding mechanisms illustrate how the ACA sought to redistribute healthcare costs, requiring higher earners and certain industries to contribute more to support broader coverage.
Employer Mandate
The employer mandate, officially known as the “Employer Shared Responsibility Provision,” imposes a financial obligation on applicable large employers (ALEs). If an ALE does not offer minimum essential coverage to substantially all full-time employees, or if the coverage offered is not “affordable” or does not meet “minimum value” standards, the employer may be subject to a penalty. This mandate represents a direct cost pressure on businesses, particularly smaller large employers, requiring them to either invest in providing compliant health insurance or budget for potential penalties. For many businesses, it standardized the expectation of employer-sponsored health benefits, ensuring more workers had access to coverage.
Economic Effects on Healthcare Providers and Industries

The ACA had ripple effects throughout the healthcare industry. Hospitals, for instance, saw a significant reduction in uncompensated care costs as more people gained insurance, translating into improved financial stability for many institutions. However, they also faced new payment models and pressures to improve efficiency. Pharmaceutical companies and medical device manufacturers initially faced new taxes, but also gained a larger insured customer base. The insurance industry adapted to new regulations, guaranteed issue requirements (meaning insurers cannot deny coverage for pre-existing conditions), and the necessity to offer plans on the exchanges, leading to market consolidation and new competitive dynamics. These changes represented both costs (compliance, new taxes) and benefits (expanded market, reduced risk of uncompensated care) for various industry players.
Measuring the ACA’s Value vs. Its Price Tag
Assessing “how much the ACA costs” ultimately requires balancing the direct financial expenditures against the benefits realized, both individually and societally. The “value” of the ACA is often debated through the lens of coverage expansion, health outcomes, and its impact on overall healthcare spending.
Increased Coverage and Access to Care
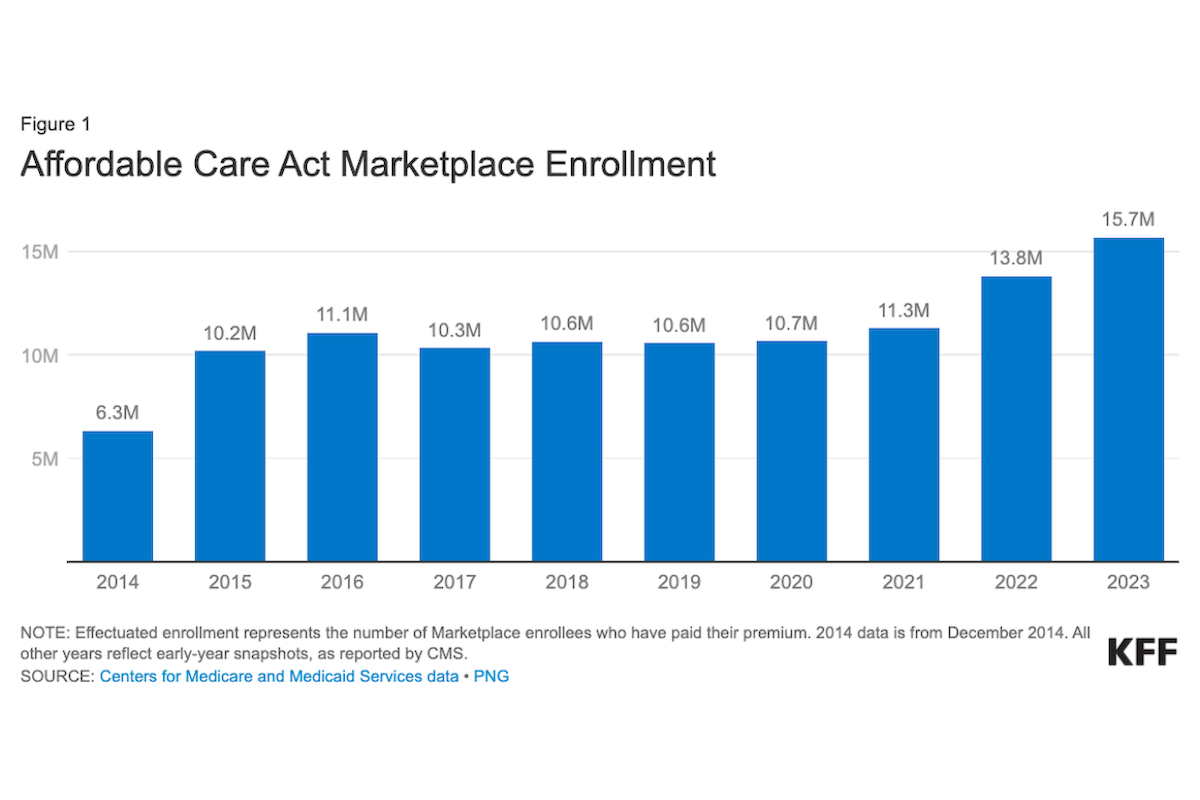
One of the most widely cited successes of the ACA is the dramatic increase in health insurance coverage. Prior to the ACA, millions of Americans were uninsured. By 2016, the uninsured rate had fallen to historic lows, with analyses attributing much of this reduction to the ACA’s provisions. This expansion meant:
- Coverage for Pre-existing Conditions: A fundamental protection, ensuring that individuals could not be denied coverage or charged more due to past or current health issues.
- Essential Health Benefits: All plans offered through the marketplaces must cover ten categories of essential health benefits, including maternity care, mental health services, and prescription drugs, ensuring comprehensive coverage.
- Preventative Care: Most plans must cover a range of preventive services, such as immunizations and screenings, without cost-sharing, promoting earlier detection and management of health issues.
- Young Adult Coverage: The provision allowing young adults to stay on their parents’ plans until age 26 significantly boosted coverage among this demographic.
The value of increased coverage goes beyond mere statistics; it translates into improved access to necessary medical care, reduced medical debt, and enhanced financial security for millions of families.
Impact on Healthcare Spending and National Debt
The question of whether the ACA “bent the cost curve” of healthcare spending remains a subject of ongoing debate. Some analyses suggest that the growth rate of healthcare spending did slow in the years following the ACA’s implementation, potentially due to aspects like payment reforms and increased emphasis on preventive care. However, overall healthcare costs in the U.S. continue to rise.
Regarding the national debt, the Congressional Budget Office (CBO) initially projected that the ACA would reduce the federal deficit over the long term, largely due to its revenue-generating provisions and slower projected growth in Medicare spending. Subsequent analyses have been more mixed, with some showing a modest deficit reduction and others indicating a slight increase, depending on the assumptions about tax revenues, subsidy costs, and changes in healthcare utilization. The ultimate impact on the national debt is a complex calculation influenced by economic conditions, legislative changes, and evolving healthcare trends.
Administrative Costs and Efficiency
Implementing and administering a law of the ACA’s scale naturally incurred significant administrative costs. This includes the establishment and operation of state and federal health insurance marketplaces, the development of complex subsidy calculation systems, and the ongoing costs of regulation and enforcement. Critics often point to these overheads as a source of inefficiency. Proponents argue that these costs are necessary investments to create a functioning and regulated insurance market that serves a broad population. Debates continue regarding the optimal balance between comprehensive regulation, market efficiency, and administrative burden.
Navigating the ACA: Practical Financial Considerations
For individuals and businesses, understanding the practical financial considerations of the ACA is key to maximizing its benefits and managing its costs.
Maximizing Subsidies and Plan Selection
Individuals shopping on the ACA marketplaces should always check their eligibility for Premium Tax Credits and Cost-Sharing Reductions. Using the official marketplace websites (HealthCare.gov or state-specific exchanges) allows applicants to accurately estimate their subsidies based on income and household size. When selecting a plan, it’s crucial to look beyond just the monthly premium:
- Metal Tier: A Silver plan is often the most cost-effective choice for those eligible for CSRs, as it provides enhanced benefits at reduced out-of-pocket costs that are not available with other metal tiers.
- Network: Ensure preferred doctors and hospitals are in-network to avoid higher out-of-network costs.
- Deductibles and Out-of-Pocket Maximums: Consider personal health needs and financial tolerance for out-of-pocket spending. A higher deductible plan (Bronze) might be suitable for healthy individuals who rarely visit the doctor, while those with chronic conditions might prefer a plan with a higher premium but lower out-of-pocket costs (Gold or Platinum).
Employer-Sponsored vs. Marketplace Plans
For many Americans, the choice is between an employer-sponsored health plan and a marketplace plan. Generally, employer plans are often more comprehensive and may have a larger portion of the premium subsidized by the employer, making them a financially attractive option. However, if an employer’s plan is deemed “unaffordable” or does not meet minimum value standards, or if an individual is eligible for significant marketplace subsidies, a marketplace plan might offer better value. It’s essential to compare total costs – premiums, deductibles, copays – for both options, factoring in any potential employer contributions or marketplace subsidies.
The Future of ACA Costs
The financial landscape of the ACA is not static. Political debates, legislative amendments, and ongoing market dynamics continue to shape its costs and benefits. Future policy decisions regarding subsidies, taxes, mandates, and regulatory oversight could significantly alter “how much the ACA costs” for individuals, businesses, and the government. Understanding these potential changes is vital for long-term financial planning related to healthcare.

Conclusion
The question “how much is the ACA?” reveals a complex interplay of individual financial decisions, government spending, economic policy, and healthcare reform. For individuals, it’s the premium paid, often offset by substantial tax credits, alongside deductibles and other out-of-pocket expenses. For the government, it represents billions in subsidies and Medicaid funding, partially offset by specific taxes and fees. For businesses, it can mean compliance costs, employer contributions, or penalties.
Ultimately, the cost of the ACA is a reflection of its ambitious goals: to expand health insurance coverage, protect consumers, and bring greater stability to the healthcare market. While the financial investment is considerable and continuously debated, the value proposition—measured in increased access to care, reduced financial risk for millions, and protections against pre-existing conditions—is a central part of the discussion. Understanding the full scope of the ACA’s financial framework is essential for anyone seeking to comprehend its enduring impact on the American economy and healthcare system.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.