NSAIDs, or Nonsteroidal Anti-Inflammatory Drugs, represent a cornerstone of modern pain management and inflammation control. Their widespread availability, ranging from over-the-counter (OTC) options to prescription-strength formulations, underscores their importance in treating a vast spectrum of ailments. From the nagging ache of a headache to the debilitating pain of arthritis, NSAIDs offer a vital therapeutic avenue. However, understanding what constitutes an NSAID, how they function, and the nuances of their application is crucial for both patients and healthcare professionals to ensure safe and effective utilization. This exploration delves into the core of NSAID therapy, dissecting their mechanisms, common examples, and the critical considerations surrounding their use.
The Biochemical Foundation of Pain and Inflammation: Understanding NSAID Mechanisms
NSAIDs are not a monolithic entity; rather, they are a diverse class of drugs unified by their fundamental mechanism of action: the inhibition of cyclooxygenase (COX) enzymes. This biochemical pathway is central to the body’s inflammatory response, pain signaling, and the maintenance of several physiological functions. To truly grasp what medications are NSAIDs, one must first appreciate this underlying science.
The Cyclooxygenase (COX) Pathways: COX-1 and COX-2
At the heart of NSAID pharmacology lies the COX enzyme family. These enzymes are responsible for converting arachidonic acid, a fatty acid found in cell membranes, into prostaglandins. Prostaglandins are potent signaling molecules that play a multifaceted role in the body. There are two primary isoforms of the COX enzyme: COX-1 and COX-2.
- COX-1: This isoform is constitutively expressed, meaning it is always present and active in various tissues. COX-1 is primarily involved in “housekeeping” functions. It plays a critical role in protecting the stomach lining by promoting the production of prostaglandins that stimulate mucus secretion and bicarbonate production, thereby neutralizing stomach acid. Furthermore, COX-1 is essential for platelet aggregation, a process vital for blood clotting.
- COX-2: In contrast, COX-2 is inducible. Its expression is significantly upregulated at sites of inflammation in response to stimuli such as cytokines, growth factors, and endotoxins. COX-2-derived prostaglandins are the primary mediators of inflammation, characterized by redness, swelling, heat, and pain. They also contribute to the sensitization of pain receptors, leading to hyperalgesia (increased sensitivity to pain).
How NSAIDs Interfere with Prostaglandin Synthesis
NSAIDs exert their therapeutic effects by competitively inhibiting the activity of both COX-1 and COX-2 enzymes. By blocking these enzymes, NSAIDs reduce the production of prostaglandins. The extent to which an NSAID inhibits COX-1 versus COX-2 dictates its therapeutic profile and its potential for side effects.
- Anti-inflammatory and Analgesic Effects: The reduction in COX-2-derived prostaglandins at the site of inflammation directly leads to decreased redness, swelling, and pain. This is the primary therapeutic benefit of NSAIDs.
- Antipyretic Effects: NSAIDs can also reduce fever. Prostaglandins, particularly PGE2, are involved in the brain’s thermoregulatory center, and their reduced production by NSAIDs helps to reset the body’s thermostat, bringing down elevated temperatures.
The Double-Edged Sword: Balancing Efficacy and Side Effects
While the inhibition of COX-2 is responsible for the desired anti-inflammatory and analgesic effects, the concurrent inhibition of COX-1 is often the cause of significant adverse reactions. This is why understanding the selectivity of different NSAIDs is paramount.
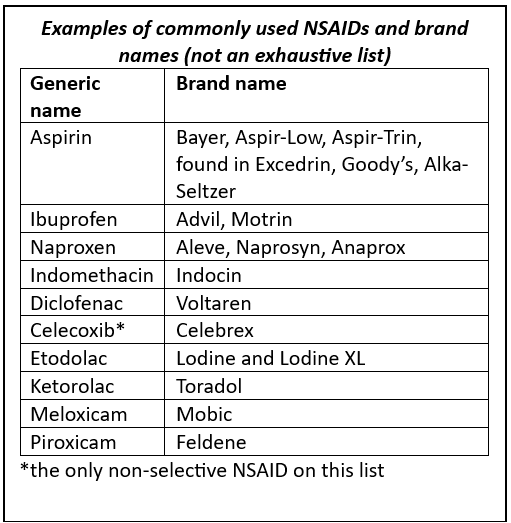
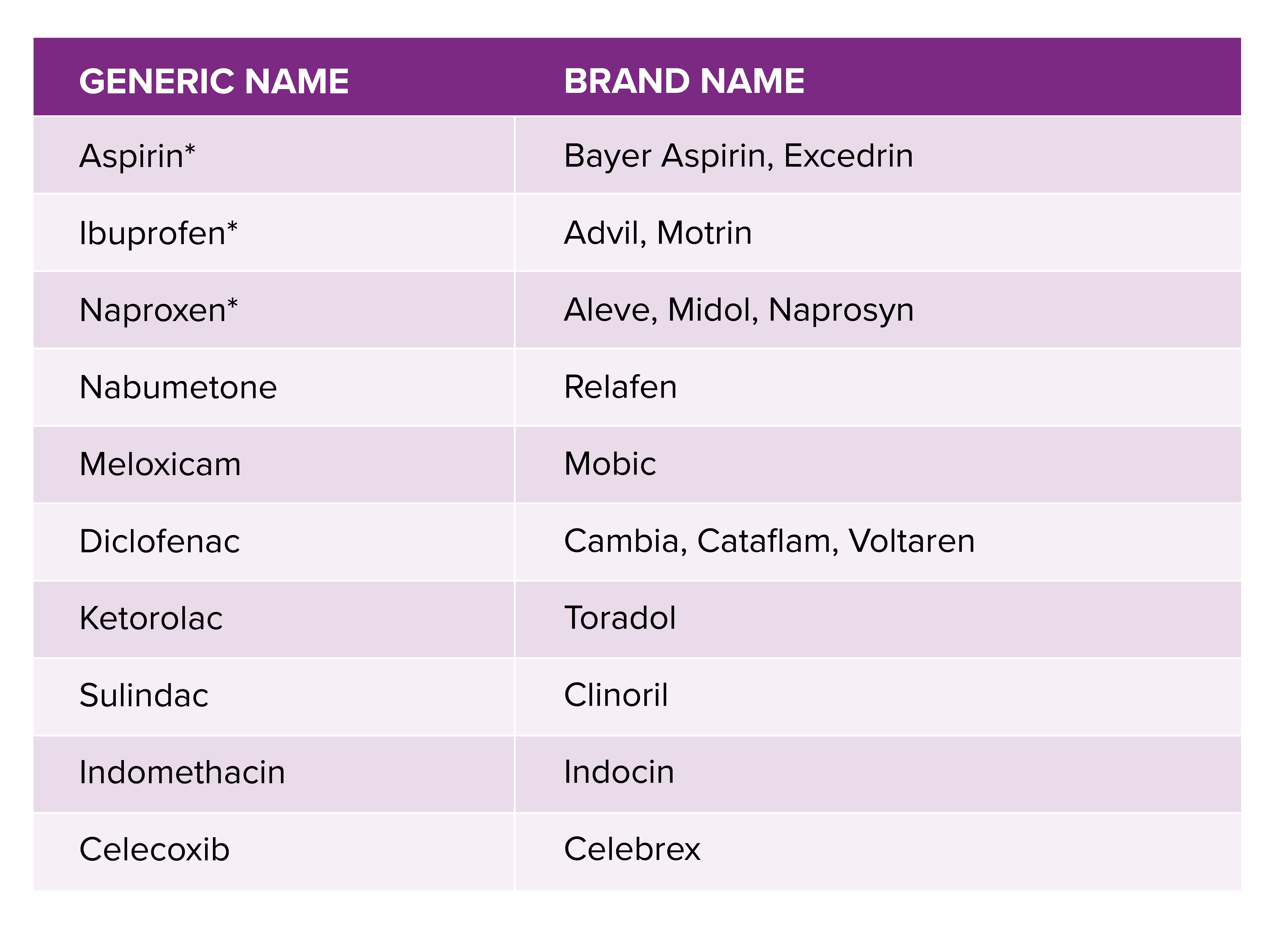
A Pharmacological Landscape: Common NSAIDs and Their Classifications
The category of NSAIDs encompasses a broad array of drugs, each with its unique chemical structure, pharmacological properties, and therapeutic applications. Categorizing these medications helps in understanding their nuances and selecting the most appropriate option for a given clinical scenario. Broadly, NSAIDs can be classified based on their chemical structure or their selectivity for COX-1 and COX-2 enzymes.
Traditional NSAIDs: Non-Selective COX Inhibitors
The majority of commonly used NSAIDs are non-selective inhibitors, meaning they inhibit both COX-1 and COX-2 enzymes to varying degrees. These have been the workhorses of NSAID therapy for decades.
- Salicylates: The oldest and perhaps most well-known NSAID is aspirin. While it exhibits some anti-inflammatory properties, its primary use at lower doses is for its antiplatelet effects, preventing blood clots in cardiovascular conditions. At higher doses, it functions as an analgesic and anti-inflammatory agent. Other salicylates exist, though aspirin remains the most prominent.
- Propionic Acid Derivatives: This is a large and very common group of NSAIDs. Examples include:
- Ibuprofen: Widely available OTC and by prescription, ibuprofen is effective for mild to moderate pain, fever, and inflammation. It’s a staple for conditions like headaches, menstrual cramps, and muscle strains.
- Naproxen: Also available OTC and by prescription, naproxen has a longer duration of action than ibuprofen, often requiring less frequent dosing. It’s commonly used for arthritis, tendonitis, and bursitis.
- Ketoprofen: Another propionic acid derivative, available both OTC and by prescription, with similar indications to ibuprofen and naproxen.
- Acetic Acid Derivatives: This group includes drugs like:
- Diclofenac: Available in various formulations, including oral, topical, and injectable. Diclofenac is a potent NSAID used for a range of inflammatory conditions, including osteoarthritis and rheumatoid arthritis. Topical formulations are particularly useful for localized musculoskeletal pain.
- Indomethacin: A potent NSAID, often used for more severe inflammatory conditions like gout and ankylosing spondylitis, but its higher incidence of gastrointestinal side effects limits its routine use.
- Oxicam Derivatives:
- Piroxicam: Known for its long half-life, allowing for once-daily dosing. It’s used for chronic inflammatory conditions but carries a higher risk of gastrointestinal issues.
- Meloxicam: While technically a COX-2 selective inhibitor, it exhibits a dose-dependent selectivity, meaning at lower doses it preferentially inhibits COX-2, but at higher doses, it also inhibits COX-1. This provides a more favorable gastrointestinal safety profile compared to non-selective NSAIDs.
COX-2 Selective Inhibitors (Coxibs): A Targeted Approach
Recognizing the significant gastrointestinal risks associated with COX-1 inhibition, pharmaceutical research focused on developing NSAIDs that selectively target COX-2. These drugs were designed to provide anti-inflammatory and analgesic benefits with a reduced risk of stomach ulcers and bleeding.
- Celecoxib: The most widely prescribed COX-2 selective inhibitor. It is indicated for osteoarthritis, rheumatoid arthritis, and acute pain. While offering improved gastrointestinal safety, concerns regarding cardiovascular risks have emerged with some COX-2 inhibitors.
- Etoricoxib, Lumiracoxib, Rofecoxib, Valdecoxib: These were also developed as COX-2 selective inhibitors, but some, like rofecoxib and valdecoxib, were withdrawn from the market due to concerns about increased cardiovascular events. This highlights the complex risk-benefit profile of even highly targeted NSAIDs.
The choice between a traditional NSAID and a COX-2 selective inhibitor often depends on a patient’s individual risk factors, particularly their gastrointestinal and cardiovascular health.
Navigating the Therapeutic Landscape: Indications and Clinical Applications of NSAIDs
The versatility of NSAIDs makes them indispensable in managing a wide array of medical conditions. Their ability to reduce pain, inflammation, and fever addresses symptoms that significantly impact a patient’s quality of life. Understanding their established indications is crucial for appropriate therapeutic use.
Pain Management: From Acute Episodes to Chronic Conditions
NSAIDs are a cornerstone of pain relief across the spectrum of pain intensity and duration.

- Acute Pain: This includes pain arising from injuries such as sprains, strains, fractures, and post-surgical pain. For mild to moderate acute pain, OTC NSAIDs like ibuprofen and naproxen are often the first line of treatment. They can effectively reduce pain and swelling, facilitating mobility and recovery.
- Chronic Pain: For chronic pain conditions characterized by inflammation, NSAIDs play a significant role.
- Osteoarthritis: This degenerative joint disease causes pain and stiffness due to the breakdown of cartilage. NSAIDs help to reduce inflammation in the joint lining (synovium) and alleviate pain, improving joint function.
- Rheumatoid Arthritis: An autoimmune disease where the body’s immune system attacks the joints, causing inflammation and damage. NSAIDs are used to manage the pain and inflammation associated with RA, though disease-modifying antirheumatic drugs (DMARDs) are essential for altering the disease course.
- Ankylosing Spondylitis: A chronic inflammatory disease primarily affecting the spine, causing pain and stiffness. NSAIDs are often the first-line treatment for symptom management.
- Gout: A form of inflammatory arthritis caused by the buildup of uric acid crystals in the joints. While specific gout medications target uric acid levels, NSAIDs are highly effective in managing the acute, severe pain and inflammation of gout flares.
Inflammatory Conditions Beyond Arthritis
The anti-inflammatory properties of NSAIDs extend their utility to various other inflammatory disorders.
- Tendonitis and Bursitis: Inflammation of tendons and bursae, respectively, often caused by overuse or injury. NSAIDs can reduce the localized inflammation and pain, aiding in recovery.
- Menstrual Cramps (Dysmenorrhea): Prostaglandins play a significant role in uterine contractions, which cause menstrual cramps. NSAIDs effectively inhibit prostaglandin synthesis, providing substantial relief from menstrual pain.
- Headaches and Migraines: While the exact mechanisms of NSAID action in headaches are complex, they can be effective for certain types of headaches, including tension headaches and mild to moderate migraines, by reducing inflammation and pain signaling.
- Post-Operative Pain and Inflammation: Following surgical procedures, NSAIDs are frequently used to manage pain and reduce swelling, contributing to a more comfortable recovery and potentially reducing the need for opioid analgesics.
Non-Pain Related Uses: A Broader Spectrum
Beyond their primary roles in pain and inflammation, NSAIDs have other established clinical applications.
- Cardiovascular Prevention (Aspirin): As mentioned, low-dose aspirin is widely used for secondary prevention of cardiovascular events like heart attacks and strokes in individuals with established cardiovascular disease. Its antiplatelet effect inhibits the formation of blood clots that can lead to these events.
- Fever Reduction (Antipyresis): NSAIDs are effective in reducing fever by acting on the thermoregulatory center in the hypothalamus. This is particularly useful in managing fevers associated with infections or inflammatory conditions.
- Certain Dermatological Conditions: In some cases, NSAIDs might be used adjunctively to manage inflammation associated with certain skin conditions, though this is less common and usually in conjunction with topical treatments.
The judicious selection of an NSAID for a specific condition requires careful consideration of the patient’s medical history, potential contraindications, and the risk-benefit profile of the drug.
Considerations for Safe and Effective NSAID Use: Balancing Benefits and Risks
While NSAIDs are powerful therapeutic agents, their use is not without potential risks. A comprehensive understanding of these risks, contraindications, drug interactions, and appropriate monitoring strategies is essential to maximize their benefits while minimizing harm. Safe and effective NSAID therapy hinges on informed decision-making and personalized care.
Gastrointestinal and Cardiovascular Risks: The Primary Concerns
The most well-documented and concerning side effects of NSAID use are related to the gastrointestinal tract and the cardiovascular system.
- Gastrointestinal (GI) Complications: Due to the inhibition of COX-1, which impairs the protective mechanisms of the stomach lining, NSAIDs can lead to:
- Gastric Ulcers: Sores that develop in the lining of the stomach or duodenum.
- GI Bleeding: This can range from occult blood loss (undetectable without testing) to severe, life-threatening hemorrhages.
- Perforation: A hole in the stomach or intestinal wall, a medical emergency.
- Dyspepsia: Indigestion, heartburn, and abdominal discomfort are common.
The risk of GI complications is higher with prolonged use, higher doses, in elderly patients, those with a history of ulcers, and those taking concomitant medications like corticosteroids or anticoagulants.
- Cardiovascular (CV) Risks: Non-aspirin NSAIDs, particularly COX-2 selective inhibitors, have been associated with an increased risk of:
- Myocardial Infarction (Heart Attack):
- Stroke:
- Heart Failure: NSAIDs can cause fluid retention and worsen hypertension, contributing to heart failure exacerbations.
The risk appears to be dose-dependent and is particularly concerning in individuals with pre-existing cardiovascular disease or risk factors. Aspirin, when used for cardioprotection, has the opposite effect.
Renal and Hepatic Effects: Less Common but Significant
While less frequent than GI or CV issues, NSAIDs can also impact the kidneys and liver.
- Renal Impairment: NSAIDs can reduce blood flow to the kidneys, potentially leading to:
- Acute Kidney Injury: Especially in patients who are dehydrated, have pre-existing kidney disease, or are taking other nephrotoxic medications.
- Sodium and Fluid Retention: Contributing to edema and hypertension.
- Hepatic Impairment: Although rare, NSAIDs can cause liver damage, characterized by elevated liver enzymes. Patients with pre-existing liver disease should use NSAIDs with extreme caution.
Contraindications and Precautions: Who Should Avoid NSAIDs?
Certain patient populations are at higher risk from NSAID therapy and should avoid them or use them only under strict medical supervision.
- Active Peptic Ulcer Disease or GI Bleeding:
- Severe Heart Failure:
- Severe Renal or Hepatic Impairment:
- Allergy or Hypersensitivity to NSAIDs: Including those with a history of aspirin-induced asthma.
- Late Pregnancy (Third Trimester): As NSAIDs can interfere with labor and delivery and pose risks to the fetus.
- Perioperative Pain in Coronary Artery Bypass Graft (CABG) Surgery: Due to increased risk of CV events.
Drug Interactions: A Complex Web
NSAIDs can interact with a wide range of other medications, potentially altering their efficacy or increasing the risk of adverse effects.
- Anticoagulants (e.g., Warfarin, DOACs): Increased risk of bleeding.
- Corticosteroids: Synergistic risk of GI ulcers and bleeding.
- Antiplatelet Agents (e.g., Clopidogrel): Increased risk of bleeding.
- Lithium: NSAIDs can increase lithium levels, leading to toxicity.
- Methotrexate: NSAIDs can increase methotrexate levels, leading to toxicity.
- Diuretics and Antihypertensives: NSAIDs can reduce the effectiveness of these medications and increase the risk of kidney damage.
Strategies for Minimizing Risks and Ensuring Safe Use
- Lowest Effective Dose for Shortest Duration: Always aim to use the lowest dose that provides adequate symptom relief and for the shortest possible period.
- Consider Patient Risk Factors: Thoroughly assess a patient’s GI, CV, and renal history before prescribing or recommending NSAIDs.
- Use Gastroprotective Agents: For patients at high risk of GI complications, co-administration of a proton pump inhibitor (PPI) or misoprostol may be considered.
- Educate Patients: Ensure patients understand the potential side effects, warning signs of complications (e.g., black stools, severe abdominal pain, unexplained weight gain), and when to seek medical attention.
- Regular Monitoring: For long-term NSAID users, regular monitoring of blood pressure, kidney function, and for signs of GI bleeding is advisable.
- Explore Alternatives: Consider alternative pain relief strategies, such as acetaminophen, physical therapy, or non-pharmacological interventions, especially in patients with contraindications or high-risk profiles.
In conclusion, NSAIDs are potent and valuable medications for managing pain and inflammation. However, their use demands a thorough understanding of their mechanisms, the diverse range of available drugs, their indications, and, critically, the potential risks involved. By adopting a cautious, informed, and individualized approach, healthcare professionals and patients can harness the benefits of NSAIDs while navigating their complexities for optimal therapeutic outcomes.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.