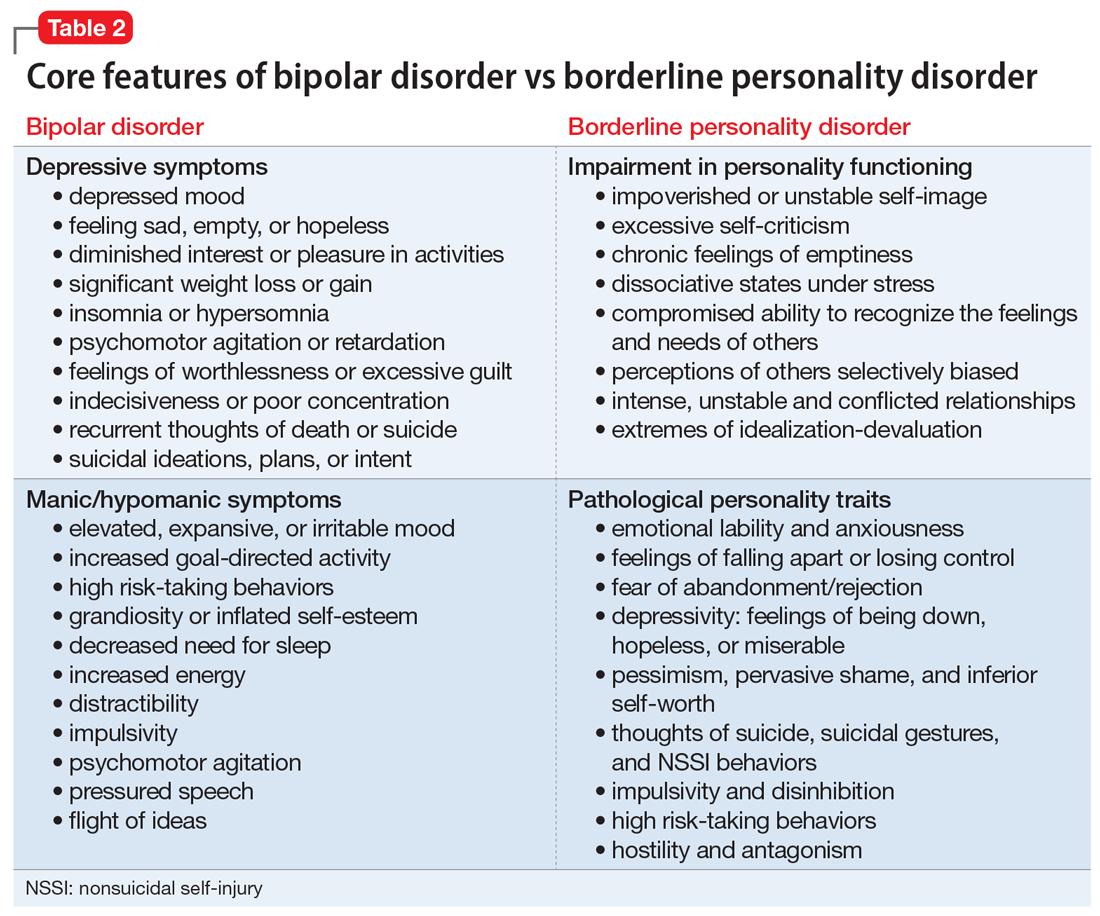
In the rapidly evolving landscape of HealthTech, the intersection of psychiatry and artificial intelligence has opened new frontiers for precision medicine. For decades, clinical practitioners relied heavily on subjective observation and patient self-reporting to distinguish between complex mental health conditions. Among the most challenging to differentiate are Bipolar Disorder (BD) and Borderline Personality Disorder (BPD). While they share overlapping symptoms—such as emotional instability and impulsivity—their underlying mechanisms and treatment trajectories differ significantly.
Today, the “difference” is no longer just a clinical debate; it is a data-driven discovery. Through the lens of advanced software, wearable telemetry, and machine learning, the technology sector is redefining how we identify, categorize, and treat these conditions. This article explores how modern technology clarifies the distinction between Bipolar and Borderline Personality Disorder through digital phenotyping, algorithmic analysis, and physiological monitoring.

The Role of AI and Machine Learning in Symptom Mapping
At the core of the technological revolution in mental health is the ability of machine learning (ML) models to process vast datasets that the human eye might miss. When distinguishing between Bipolar Disorder and BPD, AI tools focus on “temporal patterns”—the timing and duration of mood shifts.
Algorithmic Pattern Recognition in Mood Fluctuations
Bipolar Disorder is primarily characterized by episodic shifts in mood, ranging from depressive lows to manic highs. These cycles typically last weeks or months. In contrast, Borderline Personality Disorder involves “affective instability,” where moods may shift several times within a single day, often triggered by interpersonal stressors.
Software developers are now building ML algorithms capable of mapping these fluctuations with high granularity. By analyzing longitudinal data from mood-tracking apps, AI can identify the “periodicity” of a patient’s state. An algorithm can distinguish the long-wave oscillations of Bipolar mania from the high-frequency, reactive spikes associated with BPD. This mathematical distinction helps clinicians move away from “best guess” scenarios toward data-backed diagnoses.
Natural Language Processing (NLP) and Digital Phenotyping
Digital phenotyping refers to the moment-by-moment quantification of the individual-level human phenotype in situ using data from personal digital devices. One of the most potent tools in this niche is Natural Language Processing (NLP).
Tech startups are developing tools that analyze the sentiment, syntax, and frequency of a user’s digital communication (with consent). In Bipolar Disorder, manic phases often manifest as “pressured speech”—translated in the digital world as a rapid increase in post frequency, word count, and high-energy vocabulary. BPD, however, often shows a different linguistic signature: a high density of “splitting” language (absolute terms like “always,” “never,” “perfect,” or “evil”) and themes of abandonment. By processing these linguistic “fingerprints,” NLP software provides a non-invasive way to distinguish the two disorders based on digital behavior.
Wearable Technology: Tracking Biological Markers vs. Behavioral Shifts
While software analyzes what patients say and do, wearable hardware tracks what their bodies are experiencing. The difference between Bipolar and BPD is often written in the body’s circadian rhythms and autonomic nervous system responses.
Circadian Rhythm Monitoring for Bipolar Identification
One of the hallmarks of Bipolar Disorder is its profound impact on the biological clock. During a manic episode, a person may require very little sleep but remain highly energized; during a depressive episode, hypersomnia is common.
Modern wearables, such as smart rings and advanced fitness trackers, provide continuous telemetry on sleep architecture and rest-activity cycles. Tech platforms can now flag “circadian dysregulation” as a primary marker for Bipolar Disorder. If the data shows a systemic collapse of sleep patterns over a two-week period without a corresponding drop in physical activity, the tech points toward a Bipolar manic episode. This biological “signal” is much less common in BPD, where sleep disturbances are typically more sporadic and less tied to long-term cyclical shifts.
High-Frequency Biometric Data and Emotional Dysregulation in BPD
Borderline Personality Disorder is fundamentally a disorder of emotional regulation. From a tech perspective, this manifests as “autonomic hyper-reactivity.” Wearables equipped with Electrodermal Activity (EDA) sensors and Heart Rate Variability (HRV) monitors can track the body’s “fight or flight” response in real-time.
For a patient with BPD, a minor social slight might trigger a massive physiological spike—a rapid drop in HRV and an increase in skin conductance. Tech tools can map these “micro-events.” By correlating biometric spikes with GPS data (location) or calendar events (meetings/social gatherings), software can identify that a patient’s distress is reactive and situational (indicative of BPD) rather than endogenous and persistent (indicative of Bipolar).
Digital Therapeutics (DTx) and Specialized Software Solutions
Once the distinction is made, the technology sector provides specialized intervention pathways known as Digital Therapeutics (DTx). Because the “difference” between the two disorders involves different psychological needs, the software must be tailored accordingly.
Software-Led CBT vs. Dialectical Behavior Therapy (DBT)
The gold standard for BPD treatment is Dialectical Behavior Therapy (DBT), which focuses on distress tolerance and emotional regulation. Conversely, Bipolar Disorder often requires Cognitive Behavioral Therapy (CBT) focused on routine-building and medication adherence.
The tech industry has responded by creating specialized app ecosystems. DBT-focused apps like “Daylio” or “DBT Coach” utilize interactive modules that help users navigate intense emotional crises in the moment—a feature critical for BPD. Meanwhile, Bipolar-specific platforms focus on “Social Rhythm Therapy” tools, using UI/UX designs that encourage stability, medication reminders, and the avoidance of over-stimulation. This specialization ensures that the digital intervention matches the specific pathology identified by the diagnostic tools.
Data-Driven Feedback Loops for Clinicians
One of the most significant advantages of this tech stack is the creation of a “closed-loop” system. Telehealth platforms now integrate data from wearables and mood apps directly into a clinician’s dashboard.
For a psychiatrist, seeing a “heat map” of a patient’s mood over six months is far more useful than a 15-minute interview. If the heat map shows sustained periods of high energy (hypomania), the clinician can adjust mood stabilizers for Bipolar Disorder. If the map shows a “jagged” pattern of daily emotional crashes, the clinician might pivot toward psychotherapy for BPD. This tech-enabled transparency reduces the risk of misdiagnosis, which is historically high—many BPD patients are misdiagnosed as Bipolar II, leading to ineffective or even harmful medication regimens.
Challenges in Digital Diagnostics: Data Privacy and Algorithmic Bias
While the technological shift offers unprecedented clarity, it also introduces significant challenges that the tech industry must address to remain ethical and effective.
The Ethical Frontier of Mental Health Data
The distinction between Bipolar and BPD involves collecting the most intimate data imaginable: sleep cycles, location patterns, social interactions, and even the “tone” of private messages. As the Tech sector moves deeper into mental health, data security is paramount.
End-to-end encryption and decentralized data storage (Web3 applications) are becoming standard requirements for mental health startups. The challenge lies in balancing the “openness” required for AI to learn with the “opacity” required to protect patient privacy. Furthermore, there is the risk of “digital labeling,” where an algorithm’s diagnosis might follow a user across digital platforms, potentially affecting insurance premiums or employment if data leaks occur.
Refining Accuracy in Predictive Analytics
The final hurdle is the “black box” of AI. If an algorithm determines a user has BPD based on their social media usage, the developer must ensure the model isn’t simply flagging “introversion” or “creative expression” as a pathology.
The tech community is currently focused on “Explainable AI” (XAI)—models that don’t just provide a result but explain why they reached that conclusion. In the context of the Bipolar vs. BPD debate, XAI would show that the diagnosis was based on, for example, a 40% deviation in circadian rhythm rather than an arbitrary sentiment score. This transparency is vital for clinical adoption and patient trust.
Conclusion
The difference between Bipolar and Borderline Personality Disorder is a study in patterns, biology, and reactivity. Through the integration of AI, wearable biometrics, and sophisticated software, the tech industry is providing the tools necessary to move beyond clinical ambiguity. By transforming subjective experiences into objective data points, technology is not only helping clinicians make better distinctions but is also empowering patients to understand the unique rhythms of their own minds. As these tools continue to mature, the path to personalized, effective mental healthcare becomes clearer, driven by the power of digital innovation.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.