Acute appendicitis is a common surgical emergency characterized by inflammation of the appendix, a small, finger-like pouch attached to the large intestine. While often discussed in a medical context, understanding the fundamentals of acute appendicitis can empower individuals with knowledge about a potentially serious health condition, enabling them to recognize symptoms, seek timely medical attention, and appreciate the underlying biological processes. This article delves into the definition, causes, symptoms, diagnosis, and treatment of acute appendicitis, offering a comprehensive overview for a general audience.
The Anatomy and Pathogenesis of Appendicitis
The appendix, a vestigial organ in evolutionary terms, is located in the lower right abdomen, originating from the cecum, the first part of the large intestine. Its exact physiological function in humans remains a subject of debate, with theories ranging from a reservoir for beneficial gut bacteria to a role in immune system development. However, its small size and relatively simple structure do not preclude it from becoming a site of significant inflammation.

What Triggers Appendicitis?
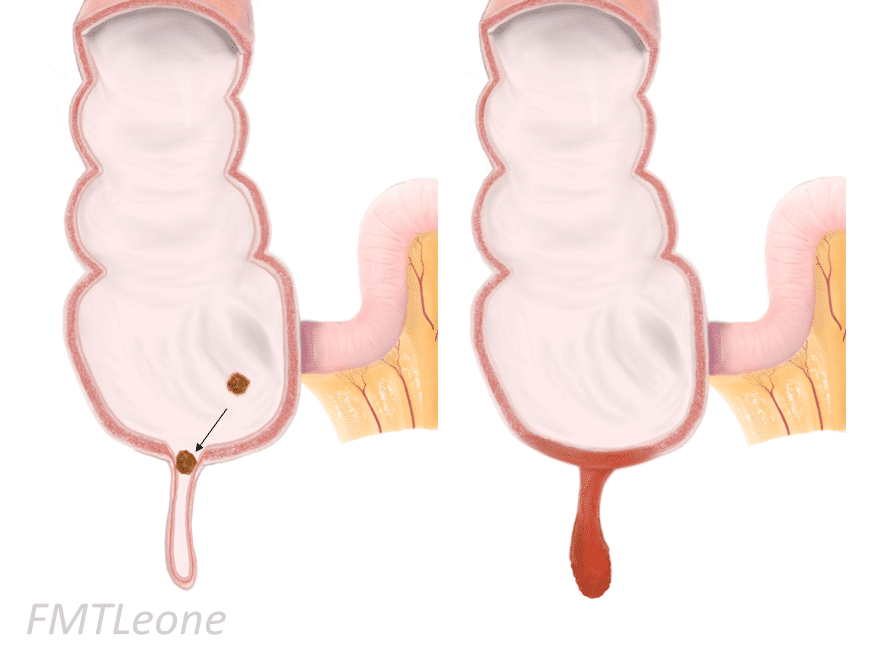
The primary mechanism behind acute appendicitis is obstruction of the appendiceal lumen, the hollow passageway within the appendix. This blockage can be caused by several factors, leading to a cascade of inflammatory events.
Common Causes of Appendiceal Obstruction
- Fecaliths: These are hardened masses of stool that can become lodged in the opening of the appendix. Fecaliths are particularly common in adults and are often composed of compacted fecal matter, undigested food particles, and calcium salts.
- Lymphoid Hyperplasia: In younger individuals, particularly children and adolescents, the lymphoid tissue within the appendiceal wall can enlarge and swell, often in response to viral infections or other inflammatory conditions. This swollen lymphoid tissue can then compress and obstruct the appendiceal lumen.
- Foreign Bodies: Although less common, ingested foreign objects such as seeds, fruit pits, or even small pieces of plastic can migrate to and obstruct the appendix.
- Tumors: In rare instances, tumors within the appendix or cecum can cause obstruction. These are more prevalent in older adults.
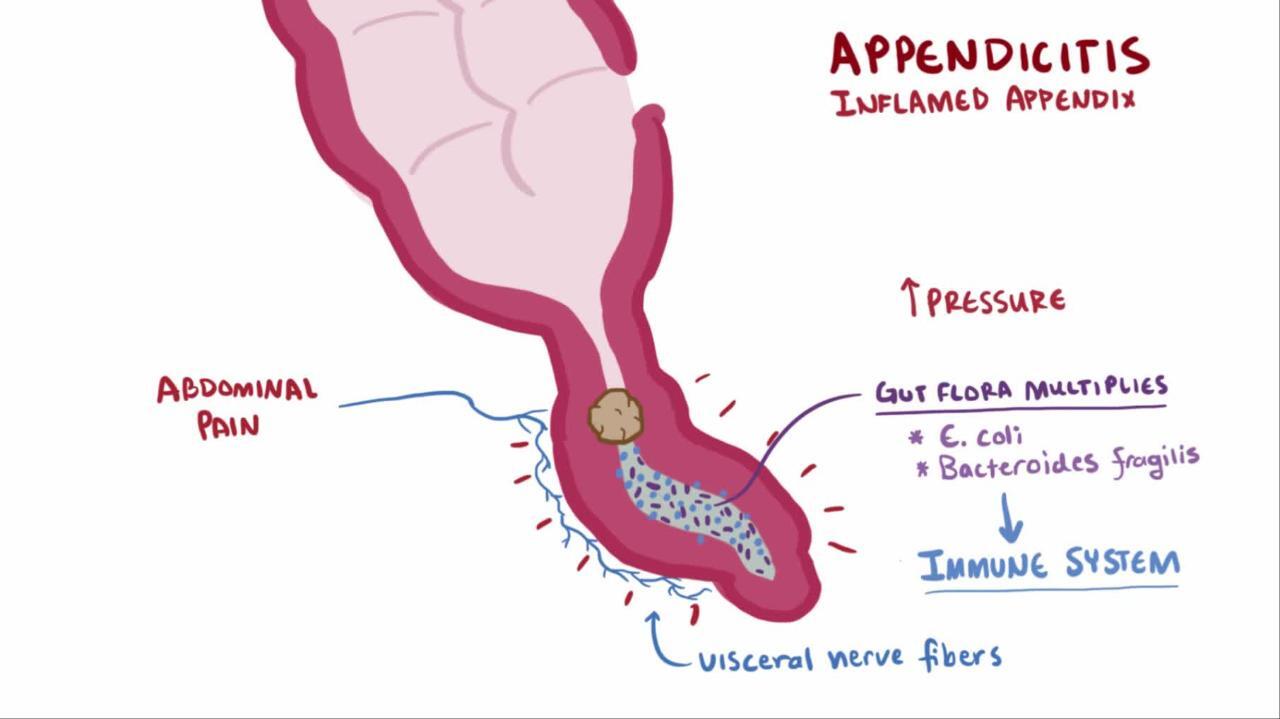
Once the lumen is obstructed, the normal flow of mucus and bacteria within the appendix is disrupted. Bacteria, normally residing in the gut, proliferate in the stagnant environment, leading to infection and inflammation. This inflammation causes the appendiceal wall to swell and become engorged with blood. As the pressure inside the appendix increases, it can compromise blood supply, leading to tissue death (necrosis) and potentially perforation.
The Inflammatory Cascade
The inflammation of the appendix, or appendicitis, is a complex biological response. When the lumen is blocked, bacteria begin to multiply. Their metabolic byproducts and the inflammatory response triggered by the body’s immune system lead to the release of various enzymes and cytokines. These substances contribute to the swelling, pain, and eventual damage to the appendiceal wall. If left untreated, the inflammation can progress, leading to a transmural (through the wall) infection. This can result in localized pus collection (abscess) or a more widespread infection of the abdominal cavity (peritonitis). Perforation is a critical complication, as it allows the infectious contents of the appendix to spill into the sterile peritoneal cavity, posing a significant threat to life.
Recognizing the Symptoms of Acute Appendicitis
The hallmark symptom of acute appendicitis is abdominal pain, but its presentation can vary significantly among individuals. Recognizing the subtle and evolving nature of these symptoms is crucial for early diagnosis and treatment.
The Shifting Landscape of Abdominal Pain
The characteristic pain of appendicitis typically begins as a dull ache in the periumbilical region (around the navel). This diffuse pain is often difficult for patients to pinpoint. Over a period of several hours, usually 12 to 24, the pain migrates and intensifies, localizing to the right lower quadrant of the abdomen, just above McBurney’s point (a point approximately one-third of the way from the anterior superior iliac spine to the umbilicus).
Characteristics of Appendiceal Pain
- Initial Diffuse Pain: As mentioned, the pain often starts centrally around the belly button and can be difficult to describe.
- Migration to the Right Lower Quadrant: The most significant indicator is the movement of this pain to the right lower abdomen. This migration is thought to be due to the visceral peritoneum (lining of the abdominal organs) initially being irritated, followed by irritation of the parietal peritoneum (lining of the abdominal wall) as the inflammation becomes more localized.
- Aggravating Factors: The pain typically worsens with movement, coughing, sneezing, or any form of abdominal palpation. This suggests an inflammatory process irritating the sensitive abdominal lining.
- Character of Pain: The pain often becomes sharper and more constant as the inflammation progresses.
Beyond Pain: Other Indicative Symptoms
While abdominal pain is the primary complaint, several other symptoms frequently accompany acute appendicitis, further aiding in its identification.
Associated Signs and Symptoms
- Nausea and Vomiting: These are common and often follow the onset of pain. The vomiting is typically not bilious (containing bile) and is usually not forceful.
- Loss of Appetite (Anorexia): A significant decrease or complete loss of appetite is a classic symptom, often preceding other complaints.
- Fever: A low-grade fever, typically between 100°F (37.8°C) and 102°F (38.9°C), is frequently present. Higher fevers can indicate complications like perforation.
- Changes in Bowel Habits: Some individuals may experience constipation, while others might have mild diarrhea. This variability is due to the inflammatory process affecting nearby bowel loops.
- Abdominal Distension: In some cases, particularly with more advanced inflammation or perforation, the abdomen may become visibly distended and feel firm to the touch.
- Urinary Symptoms: Mild pain or discomfort during urination can occur if the inflamed appendix irritates the bladder or ureter.
It’s important to note that not all individuals will experience all of these symptoms, and the order and intensity can vary. This is why a thorough medical history and physical examination are vital.
Diagnosing Acute Appendicitis: A Multi-faceted Approach
The diagnosis of acute appendicitis relies on a combination of clinical assessment, laboratory tests, and imaging studies. Given the potential for complications, a prompt and accurate diagnosis is paramount.
The Clinical Examination: A Doctor’s First Steps
A physician’s initial assessment involves a detailed discussion of the patient’s symptoms and a thorough physical examination of the abdomen.
Key Elements of the Clinical Assessment
- History Taking: The doctor will inquire about the onset, location, character, and progression of the pain, as well as the presence of associated symptoms like nausea, vomiting, and fever.
- Abdominal Palpation: This is a crucial part of the physical exam. The doctor will gently press on different areas of the abdomen to assess for tenderness, guarding (involuntary tensing of abdominal muscles), and rebound tenderness (pain that is worse when pressure is released). Specific signs like McBurney’s point tenderness, Rovsing’s sign (pain in the right lower quadrant when the left lower quadrant is palpated), and the psoas sign (pain elicited by extending the hip) are suggestive of appendicitis.
- Vital Signs: Checking temperature, heart rate, and blood pressure can provide further clues about the severity of the inflammation.
Laboratory Investigations: Uncovering the Inflammatory Markers
Blood tests play a significant role in supporting the diagnosis of appendicitis by identifying signs of inflammation and infection within the body.
Common Blood Tests
- Complete Blood Count (CBC): A CBC typically reveals an elevated white blood cell count (leukocytosis), particularly an increase in neutrophils (neutrophilia). This indicates the body’s immune system is actively fighting an infection or inflammation.
- C-Reactive Protein (CRP): CRP is a protein produced by the liver in response to inflammation. Elevated CRP levels are commonly seen in appendicitis.
- Urinalysis: A urinalysis is performed to rule out other conditions that can mimic appendicitis, such as urinary tract infections or kidney stones, which can cause flank or abdominal pain. In some cases, mild abnormalities in the urinalysis may be seen in appendicitis due to proximity to the bladder.
Imaging Modalities: Visualizing the Appendix
When clinical suspicion for appendicitis is high but not definitive, or to confirm the diagnosis and assess for complications, imaging studies are employed.
The Role of Imaging in Diagnosis
- Ultrasound: Abdominal ultrasound is often the first-line imaging modality, especially in children and pregnant women, as it does not involve radiation. It can visualize an enlarged, thickened, and non-compressible appendix, as well as surrounding fluid collections. However, its accuracy can be limited by factors such as body habitus and bowel gas.
- Computed Tomography (CT) Scan: CT scans are highly accurate in diagnosing appendicitis and are considered the gold standard in many cases, particularly in adults. A CT scan of the abdomen and pelvis can clearly delineate the appendix, identify signs of inflammation, and detect complications like abscess formation or perforation. Contrast material is often used to enhance visualization of the appendiceal wall and surrounding tissues.
- Magnetic Resonance Imaging (MRI): MRI is another non-invasive imaging technique that can be used, particularly in pregnant women when ultrasound is inconclusive, to avoid radiation exposure. It provides detailed images of the abdominal organs and can effectively diagnose appendicitis and its complications.
Management and Treatment of Acute Appendicitis
The definitive treatment for acute appendicitis is surgical removal of the inflamed appendix, a procedure known as an appendectomy. Timely intervention is crucial to prevent serious complications.
The Surgical Imperative: Appendectomy
Appendectomy is a well-established and generally safe procedure, with significant advancements in surgical techniques over the years.
Surgical Approaches
- Laparoscopic Appendectomy: This minimally invasive approach involves making several small incisions in the abdomen. A laparoscope (a thin tube with a camera) and specialized surgical instruments are inserted through these incisions to visualize and remove the appendix. Laparoscopic surgery typically results in less pain, shorter hospital stays, and faster recovery times compared to open surgery.
- Open Appendectomy: This traditional approach involves a larger incision in the right lower quadrant of the abdomen to directly access and remove the appendix. Open appendectomy is often preferred in cases of severe appendicitis with significant inflammation, perforation, or abscess formation, where a more direct view and manipulation of the inflamed tissues are necessary.
Post-Operative Care and Recovery
Following appendectomy, patients typically experience a period of recovery during which they are monitored for pain management, wound healing, and potential complications.
Expectations and Recovery Timeline
- Pain Management: Post-operative pain is managed with analgesics. The level of pain and the need for medication will vary depending on the surgical approach and the extent of inflammation.
- Dietary Progression: Patients are usually started on clear liquids and gradually progress to solid foods as their bowel function returns and they tolerate oral intake.
- Mobility: Early mobilization is encouraged to prevent complications such as blood clots and pneumonia.
- Hospital Stay: For uncomplicated laparoscopic appendectomies, hospital stays are typically brief, often one to two days. Open procedures or those with complications may require longer hospitalization.
- Return to Activities: Most individuals can return to their normal daily activities within one to two weeks after a laparoscopic appendectomy and several weeks after an open procedure. Strenuous physical activity should be avoided for a longer period as recommended by the surgeon.
The Threat of Complications
While appendectomy is highly effective, delays in diagnosis or treatment can lead to significant complications.
Potential Complications of Untreated Appendicitis
- Perforation: This is the most serious complication, where the inflamed appendix ruptures, spilling infectious contents into the abdominal cavity.
- Peritonitis: The inflammation and infection of the peritoneum, the lining of the abdominal cavity, which can be life-threatening.
- Abscess Formation: A localized collection of pus can form around the appendix or within the abdominal cavity.
- Sepsis: A life-threatening systemic inflammatory response to infection, which can occur if peritonitis is not adequately treated.
In conclusion, acute appendicitis is a common yet potentially serious condition that requires prompt medical attention. Understanding its causes, recognizing its varied symptoms, and appreciating the diagnostic and treatment approaches are vital for safeguarding one’s health. While the appendix may seem like a simple organ, its inflammation can lead to significant distress and necessitates swift, evidence-based medical intervention.
aViewFromTheCave is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Amazon, the Amazon logo, AmazonSupply, and the AmazonSupply logo are trademarks of Amazon.com, Inc. or its affiliates. As an Amazon Associate we earn affiliate commissions from qualifying purchases.